I need to review and improve my paper: introduction grammatical errorsintext citations (highligted in the paper)APA format (professor is very strict on this)conclusions is too short review refere
Running head: OPIODS USE IN THE HEALTH CARE SYSTEM
Opiods Use in the Health Care System
Marlon Parra
Virginia Lombardo
Osmani Ramirez
Jesus Diaz
Heriberto Rodriguez
Giselle Milian Vizoso
Ayosent Balart
Maria Del Carmen Leon
Carlos A Leon
Miami Regional College
Professor James
March XX, 2019
Introduction
Opioid analgesics are powerful pain-relieving medications that involve prescription such as hydrocodone, morphine, and oxycodone among other drugs while some other opioid medications have also been approved for cough treatment. Even though they have benefits as powerful analgesics, opioid misuse and abuse have significantly escalated in the United States within the past two decades and this has represented it as one of the major public health concerns due to its associated risks of coma and fatal respiratory depression as a result of opioid analgesic overdose. Various scholars have carried out studies regarding issues associated with opioid while legislatures have also been coming up with policies to address the issue. This essay is therefore going to address the recent healthcare legislature, literature review, and statistical data related to opioid as well as the role of nurses in passing the opioid legislature.
Recent Healthcare Legislature
Deaths linked to drug overdoses or misuses have lent to an unprecedented reduction in life expectancy within the United States over the past few years. According to Jukiewicz et al. (2017), opioid analgesics such as OxyContin, Percocet, and Vicodin are the most commonly prescribed drugs within the United States, with overall sales of about 2 billion dollars in a single year. This drug is however abused or misused for various reasons. Even though not every opioid user is looking for a prescription with the purpose of misusing or abusing it, there are several behaviors that are common in those who abuse it. One of the common sign of misuse and abuse is that people with no legitimate job regularly offer money for prescription drugs. According to the research conducted by National Association of Drug Diversion Investigators in 2017, oxycodone costs about 1 dollar for just a milligram in the black markets nearly anywhere within the United States (Institute for Clinical and Economic Review, 2017).
Within 2017 alone, there were more than a total of 70,000 deaths that were related to overdose deaths which accounts for more fatalities than HIV, gun violence, and auto accidents put together (Institute for Clinical and Economic Review, 2017). The opioid epidemic greatly contributed to the step up of these deaths making it to be declared a National Public Health Emergency in 2017 (Institute for Clinical and Economic Review, 2017). The United States Senate thus passed legislation in response to the opioid crisis which included more than 70 individual bills such as Health, Education, Finance, Labor, and Pensions; Commerce; Judiciary; Finance and Banking.
The Opioid Crisis Response Act of 2018 furnishes state and local authorities with resources and efficiency for fighting the opioid epidemic. This legislation is the product of 7 bipartisan hearings on opioid crisis with the Centers for Disease Control and Prevention (CDC), the Food and Drug Administration (FDA), the National Institutes of Health (NIH), the Substance Abuse and Mental Health Services Administration (SAMHSA), the Departments of Education and Labor, experts, governors, and families. This legislation provides for a broadened treatment and recovery options, considering also some changes to Medicaid and Medicare, and enhancing prevention by covering prescription practices and patient and health care provider education. Since it also takes steps to speed up and sustain research and innovation, there are several provisions within the act which aims at enhancing data-collection capabilities and the safe monitoring of drug use and trends (NASADAD, 2018).
Other provisions of the Opioid Crisis Response Act of 2018 also covers drug packaging and safety, law enforcement, and the empowerment of the Office of National Drug Control Policy and Department of Justice funding for drug courts. Opioid packaging will assist in encouraging responsible prescription behavior and reduce overprescribing, and this clarifies the authority of FDA to demand drug producers to package certain drugs, including opioids, for specified treatment durations. The act also improves FDA and Customs Border Protection (CBP) coordination along the federal border. Promoting border security will help in improving FDA’s ability to find and take over proscribed drugs like fentanyl at the border and this toughens skillful and effective coordination activities with CBP. Improving FDA and CBP coordination at the border also provides that FDA has access to modern detection technology and testing equipment so as to make it easier for a near-real-time information sharing, laboratory capacity, and upgraded facility and physical infrastructures (NASADAD, 2018).
Recovery and treatment is one of the key areas of interest of this legislation due to its provisions that institutes detailed opioid recovery centers and increasing accessibility to medication-aided treatment. There is also emphasis on the family-centered treatment and recovery and assistance for youth. Cures Grant Changes for instance focuses on federal funds on parts of the country that have been greatly affected by the opioid crisis. This will allow HHS to issue extra funding to states with the greatest age-adjusted death rate related to opioid use disorders. This provision also grants states and Tribes to channel funds to local requirements linked to substance use/abuse disorders, educate health practitioners to forbid diversion of controlled substances, and effectively utilize the funds until they are finished, instead of calling for states to use them within the financial year (NASADAD, 2018).
So as to help the state response, the bill provides 500 million dollars funding annually up to 2021 to empower and build on a state-aimed grant program instituted under the 21st Century Cures Act (NASADAD, 2018). The Cures Act funding has been utilized by states to broaden dolophine hydrochloride treatment, link individuals to the community-based treatment, assist an opioid crisis helpline, allow for medication-assisted treatment within the criminal justice setup, and broaden the availability of naloxone which is a medication used to undo overdoses. Recovery Housing Best Practices within this legislation assist those recuperating from an opioid addiction with housing and this requires HHS to issue relevant practices for entities running recovery housing facilities while Alternatives to Opioids support hospitals and other acute care entities in seeking management of pain without necessarily using opioids. The need for alternatives to opioid would therefore require the Secretary of HHS to render technical assistance linked to the use opioid alternatives, even for the general painful conditions and specific patient populations like aged patients, pregnant women, and children (NASADAD, 2018).
The legislation also made some alterations to how Medicaid resources can be applied in combating the epidemic. One key provision lifts the exemption for the institutions for mental disease (IMD), which has ever since prohibited states from using federal Medicaid funds to pay off mental health treatment in facility with inpatient beds above 16 (NASADAD, 2018). The policy was initially established with an attempt to relocate treatment away from psychiatric hospital wards. However, experts in the recent years have questioned the impact of this policy on adult Medicaid beneficiaries’ accessibility to inpatient mental health services. The unexpected rise in deaths related to drugs and the resulting demand for substance use disorder and mental health treatment options have also led many to call for this prohibition to be lifted. The new legislation therefore allows a state Medicaid program to annul the ban for adult beneficiaries with opioid use disorders. This will allow Medicaid to settle for up to 30 days of care for every beneficiary each year up to 2023 (NASADAD, 2018).
The bill also includes preparation contrived to minimize the danger of opioid use disorder by people in Medicare. It expands the use of telehealth services for treatment of opioid use and other substance disorders and authorizes a thorough screening for opioid use disorders. The legislation also demands that physician and other health care providers to apply electronic prescription for regulated substances to promote tracking. The relative magnitude of the opioid epidemic and its forceful influence on families and the entire nation are simply too outstanding to ignore and that is why the state and federal are coming up even with better legislation to address it.
Literature Review Regarding the Issue
There are also several research studies that have been conducted regarding opioids. Among such research in this essay paper includes that of Abenaa Acheampong Jones along with his team and the investigation research by Lainie Rutkow and his team and that of Shannon Miller. Jones et al. in 2017 conducted a research named “The prescription opioid use, illicit drug use, and sexually transmitted infections among participants from a community engagement program in north Central Florida.” This research by Jones et al. was motivated by the fact that Alachua County is one of the prominent counties within North Central Florida where there are higher significant rates of chlamydia and gonorrhea infections as compared to the national and state infection levels with also the highest rates of other STIs and high drug trafficking (Jones et al., 2017). The research analysis therefore examined the intersection between prescription of opioid use, illegal drug use, and STIs among Alachua County participants. The research was carried out by interviewing 2,194 Alachua County community members by Community Health Workers so as to come up with demographic surveys characteristics, health risk factors and health conditions.
( which study missing in text citation) Research found out that among 2,194 participants, 9.3% said that at one time they had an STI, 40% admitted to have used opioid prescription, while 53% reported using illicit drug. Individuals who reported using proscribed drug or illegal drug prescription were 2.89 times and 4.12 times as likely to report one or more STIs infections respectively as compared to those who have never used any of these drugs. This analysis shows that reporting one or more lifetime STI infection was greatly linked to lifetime illicit drug use with or without lifetime usage of prescription opioids if other socio-ecological variables are kept constant. The results also gave further help for the intersection of substance use with the combination of illegal drug use and prescription opioid use. (in text citation)
Rutkow et al. (2015) On the other hand carried out an investigation on “The Effect of Florida's Prescription Drug Monitoring Program and Pill Mill Laws on Opioid Prescribing and Use.” The relevance of this investigative research by Rutkow et al. is that Prescription Drug Monitoring Program (PDMP) and pill mill laws are among the principal means that states apply to minimize prescription drug abuse and diversion though there are little evidences which are in place regarding their effectiveness. The research therefore intended to measure the effectiveness of PDMP of Florida and pill mill laws on the overall and high-risk opioid prescription and use. Since state-based PDMP and pill mill laws have been the key policy methods used to address prescription drug abuse and diversion, the researchers therefore applied comparative non continuous time-series analyses to qualify changes connected with these laws in opioid prescription and usage in Florida. This research was conducted in Florida State owing to the fact that it is a state with high levels of injuries and deaths related to opioid.
(in text citation)Research found out that the joint policies were linked to modest or small scale reductions in the overall opioid volume, the average MME for each transaction, and the overall number of opioid prescriptions distributed though with no evident effect on the treatment duration (Rutkow et al., 2015). Even though their research was somehow restricted to patients and prescribers with the most prominent baseline opioid use and prescription, the results are however useful given that there is a rising rates of prescription opioid abuse and outstanding roles played by laws in changing the responses of states to the epidemic.
The lately printed ecological research involving data from the Automation of Reports and Consolidated Orders System (ARCOS) from 1999 to 2008 also established that PDMPs had no general effect on the per capita dispensing of MMEs. The research also illustrated that the PDMP and pill mill laws impacts dramatically varies between states and this can somehow be explained by wide differences in states’ PDMPs. The research by Rutkow et al. therefore included Georgia and Florida as comparability states. The other results from ecological study using ARCOS data ranging from 1997 to 2003 also proposed that PDMPs were linked with reductions in quantity of oxycodone shipments(in text citation)
The investigation by Rutkow et al. also lends to the rising evidence base assessing state policies planned to eliminate epidemic rates of opioid prescribing. Their findings suggested that PDMP and pill mill law implementation together was connected with diminutions in the mean MME in each transaction between patients and prescribers with the greatest baseline usage in Florida comparative to Georgia as a comparison state. Their research study thus showed that execution of Florida’s PDMP and pill mill law was connected to modest decline in opioid use and prescribing among patients and providers with higher levels of opioid use at baseline as compared to Georgia. All the same, owing to the large variance in PDMP operation, the generalizability of the results is probably confined to states with similarly planned PDMPs, sociodemographic profiles, and pill mill laws. In conclusion, the research by Rutkow et al. found out that to lessen the intensity of epidemic rates of prescribing, morbidity, and mortality associated with opioid abuse and diversion, the states must spend a lot of money in enforcing policies designed to lower the undue dispensing of these products.
The last literature review for this essay was done by Shannon Miller who conducted a research labelled “A Systematic Review: The Opioid Epidemic”. Miller therefore on a broader perspective examined academic literature dealing with the opioid abuse and addiction problems. This involved looking at the opioid problem’s extent and inherent reasons, as well as the effectualness of educational and other intervention methods. Miller’s reviewed literature shows that the opioid epidemic problem extends within the urban and rural communities over the entire United States and Canada. It also indicates that opioid abusers must have begun substance abuse at a comparatively younger age, and that misuse of prescription opioids is usually an arbitrate step to abuse of other drugs like heroin(in text citation)
Miller’s (in text citation)reviewed literature shows that programs for educating physicians and other health care professionals increases their disposition to take action in dealing with patients’ opioid abuse problems. He also establishes impacts that post-usage clinical and social interventions have in mitigating the opioid problem though the impacts of interventions sometimes are not effective. The reviewed literature also reveals that attempts to reduce and end opioid abuse have accomplished mixed outcomes. Other programs aiming at minimizing and stopping opioid abuse have for instance brought forth positive results while some have not. Miller (in text citation) argues through his review that even though there is a unanimity that early anti-abuse training is vital and that issuing a sustained assemblage of multi-dimensional programs can be efficient, there is still the need of the agreement as to what interventions are most probable to be efficient in halting opioid abuse before it begins.
Statistical Data Related to the Issue
Centers for Disease Control and Prevention in 2018 produced a detailed annual surveillance report of drug-related risks and outcomes in the United States that provides some relevant statistical data on opioid. These data from the annual surveillance report summarizes the most current information at the national level for drug prescription patterns, drug use, and nonfatal and fatal overdoses related to the current drug overdose epidemic. These data intends to serve as a reliable resource for persons or institutions that are tasked with addressing the ongoing national crisis on opioid and other epidemics (in text citation)
The first data is on the total number and rate of opioid prescriptions dispensed per 100 persons annually in the United States in 2017. Opioid prescriptions identified using the National Drug Code for this report included; codeine, fentanyl, hydrocodone, hydromorphone, methadone, morphine, oxycodone, oxymorphone, propoxyphene, tapentadol, tramadol, and buprenorphine(in text citation)
| Opioid prescriptions | Number | Rate per 100 persons |
| All Opioids | 191,146,822 | 58.5 |
| Opioids that are long acting or extended release | 17,442,895 | 5.3 |
| Days of supply per prescription | ||
| < 30 days | 110,759,830 | 33.9 |
| ≥ 30 days | 80,386,991 | 24.6 |
| Average opioid prescription per patient | 3.4 | |
| Average days of supply per prescription | 18.3 |
Table 1 showing data is on the total number and rate of opioid prescriptions dispensed per 100 persons annually in the United States in 2017. Data retrieved from CDC 2018 Annual Surveillance Report of Drug- Related Risks and Outcomes - United States.
The second data is on the percentage of persons who had at least one prescription filled for an opioid by sex. It showed that there were 14.8 percent of males and 19.9 percent of females who had at least one prescription filled for an opioid. (in text citation)
In terms of age, CDC found out that people above 65 years have higher chances of having at least one prescription filled for an opioid by approximately 26.8 percent followed by people within the age group of 55 to 64 who are at 26.3 percent and this trend decreases towards lower age groups. The other significant data on the opioid prescribing practices conducted by CDC shows that there is an increasing trend on the average days of supply per opioid prescription. (in text citation)
The CDC Injury Center calculation also makes it possible for various researchers to identify and classify the types of drugs that are involved in an overdose, how they are frequently involved, and how the involvement varies over time. Understanding drug involvement can also help in identifying relevant prevention and response activities. Using the CDC data, there were more than a total of 17,000 deaths involving opioids prescription in 2017, and this is equal to approximately 46 numbers of deaths each day. This number can also be an undercount of deaths connected to prescription opioids since the calculation does not comprise the deaths that are associated with other synthetic opioids also used as pain medications such as pharmaceutical fentanyl and tramadol(in text citation)
This is because over the recent years, the data have indicated that the rise in overdose deaths is being promoted by deaths involving synthetic opioids which are highly associated with illicitly manufactured fentanyl (IMF). Therefore, a large ratio of the rise in overdose deaths can reasonably be assumed to be as a result of IMF and not prescription opioids even though the updated information reported concerning overdose deaths in NVSS does not differentiate pharmaceutical fentanyl from IMF (Centers for Disease Control and Prevention, 2018).
The figure below shows the age adjusted rates of overdose deaths by drug class and year from 1999 to 2016 in the US
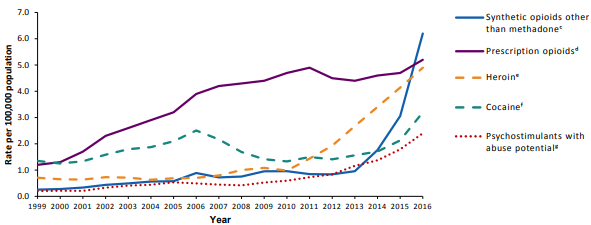
Figure 1; Overdose deaths by drug class, Retrieved from CDC 2018 Annual Surveillance Report of Drug- Related Risks and Outcomes - United States.
As per the National Institute on Drug Abuse which is a part of the National Institutes of Health, about 71 percent of diverted prescription drugs are got from a friend or relative, either free of charge which accounts for 54.2 percent or through stealing or purchase which approximates to 16.6 percent (Jones, et al. 2014). Another statistic also indicates that Americans aged 12 and above have reported that they have used illegal drug for the first time which approximates to about 2.8 million people in the United States (Jukiewicz et al., 2017). This approximation shows that there are nearly 7,800 new illegal drug users each day (Jukiewicz et al., 2017). Nearly 54.1 percent of initial illicit drug addicts started using drug abuse before turning 18 years old with the largest number of new users being females which approximated to 58 percent (Jukiewicz et al., 2017).
Again, approximately 12.5 percent proscribe drug addicts were brought in to them via other means that were no related to medical use of pain killers’ prescriptions (Jukiewicz et al., 2017). In a similar manner, CDC also posits that about 12.5 million Americans who are above 12 years have at least used opioids for purposes that were not in any way related to medical purpose which is a show of significance of the opioid epidemic. In 2007 alone as per Crowley et al.’s findings, it showed that the burden on the economy of the United States due to opioid prescription abuse was about 200 billion dollars (Philips, 2012). This economic strain included medical expenses, workplace productivity loss, and criminal and related court costs. It is due to these opioid deaths and economic burdens that the local, state, and federal government bodies have come up and established legislations that are aiming at reducing opioid overdose and opioid misuse. An example of such government effort to eliminate opioid abuse and deaths involves state registries to monitor opioid usage.
Nursing Role in Passing the Legislature
Nurses or any health care providers have a significant role to play in the implementation of the laid legislation. They can for instance assist in the prescribers' determination of how to suitably manage pain by following the results like signs, the level of patient’s consciousness, and even the overall health status of the patient. It is also a must that nurses be engaged in policy and practice initiatives at any institutional level concerning the pain scales adoption and pain interventions which are appropriate culturally and linguistically (Dahn, 2016). The following are some of the actions that can be taken by nurses to help in the implementation of legislation on opioids;
Nurses can intervene in opioid abuse by teaching patients on the dangers of opioid diversion and nonmedical use. This should entail teachings such as telling the patient that prescription medications should only be taken as per the prescription instruction and that prescription drug should never be used for any other reasons apart from the one for which they are prescribed (Dahn, 2016). Patients should also be enlightened that medications are only prescribed for the use by one person such that they cannot be used by other persons apart from the patient, even if another person exhibits the same sickness symptoms.
Controlled Substances Act also declares it a federal crime to share or take prescription medication, and therefore sharing or taking prescription medication is not just hazardous but also a violation of the Controlled Substances Act (Dahn, 2016). Another key point patient should be taught by nurses is that prescription medications, particularly those drug or substance whose use and possession is controlled by law, should be secured and only made available for the specific use by the individual to whom it was prescribed in order to prevent diversion. These teachings address the concern that most of the diverted opioids are freely offered from friends or relatives whom it was legitimately prescribed or sometimes they are stolen or sold. Educational efforts by nurses to the patients and their family members should also aim at encouraging them to secure and monitor such medications (in text citation)
Nurses can also provide education on controlled substance disposal. In the context of clinical practice, medication certification and balancing require patients to carry with them their prescriptions during their visits to their respective health care provider. Nurses can thus take advantage of such visits to teach patients to dispose and on the convenient disposal methods for the prescribed pain medications immediately they are no longer useful. The U.S’ Drug Enforcement Administration (DEA) distinguishes opioids as one of the medications that can particularly be harmful since just a single dose of it, if taken by unintended person or individual apart from the patient for whom it was prescribed, can be lethal. There has also been a common practice of disposing such medications by flushing them down the sink or toilet which Environmental Protection Agency has considered as a water supply contamination method. FDA thus only recommends a disposal via flushing if the medicinal drug "cannot be disposed of through a medicine take-back program" (Manworren & Gilson, 2015).
Nurses and nursing institutions can also help in tracking opioid use. There are however no accepted standard for monitoring opioid use mostly the short-term use for acute painful conditions but in order to limit the possibility for drug diversion, the FDA urges keeping check on the adhesion of patients getting extended-release and long-active opioids through PDMPs when indicated (Manworren & Gilson, 2015). There is also the variance among state PDMPs concerning the administering agency that has access on patient information, the way and frequency on how prescribing information is accounted and availed to users (Manworren & Gilson, 2015).
A number of organizations have also therefore published documents that outline recommended program that can promote the consistency of PDMP functions and these recommendations include; real-time data submission, data access at the point of care, integration with the electronic health record, interstate data sharing, expanded user access to data, including the authorization of delegates, maintenance of data security and confidentiality, user education, and development of valid patient risk scoring methods (Prescription Monitoring Program Center of Excellence, 2012).
Conclusion
In conclusion, the essay has seen that opioid is an addictive drug that not only helps in medicinal purpose but contributes to large number of deaths. Various statistical data from various researches have also comprehensively related opioid to various issues such as its association with some STIs. To eliminate epidemic rates of prescribing, morbidity, and mortality associated with opioid abuse and diversion, state and federal governments have spent millions of dollars to implement policies designed to curb excessive dispensing of these products. One of such policy is the implementation of The Opioid Crisis Response Act of 2018. The legislation furnishes state and local authorities with resources and efficiency for fighting the opioid epidemic. This legislation however cannot be effectual without the input of nurses and the nursing organizations. Nurses and the nursing organization represent a remarkable force that can offer education and advocacy efforts to address the opioid epidemic. (conclusion is too short)
References (please check reference APA format)
Centers for Disease Control and Prevention. 2018 Annual Surveillance Report of Drug-Related Risks and Outcomes - United States. Surveillance Special Report. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. Published August 31, 2018. Accessed [date] from www.cdc.gov/drugoverdose/pdf/pubs/2018-cdc- drugsurveillance-report.pdf
Dahn, J. (2016).The Nurse’s Role in the Opioid Crisis, Arizona Nurse, 69(4), 1
Jukiewicz, D.A., Alhofaian, A., Thompson, Z. and Gary, F.A. (2017). Reviewing Opioid Use, Monitoring, and Legislature: Nursing Perspectives, International Journal of Nursing Sciences, 4, 430 - 436
Jones, A.A., Striley, C.W. and Cottler, L.B. (2017). Prescription Opioid Use, Illicit Drug Use, And Sexually Transmitted Infections Among Participants From A Community Engagement Program In North Central Florida, Journal of Substance Use, 22(1), 90–95 DOI: 10.3109/14659891.2016.1144805
Jones S, et al. (2014) Popping Pills: Prescription Drug Abuse In America. Bethesda, MD: National Institute on Drug Abuse. http://www.drugabuse.gov/related-topics/trends- statistics/infographics/popping-p
Institute for Clinical and Economic Review (2017). Abuse Deterrent Formulations of Opioids: Effectiveness and Value https://icer-review.org/wp- content/uploads/2016/08/NECEPAC_ADF_PublicComments_062817.pdf
Manworren, R. and Aaron, G. (2015). Nurses’ Role in Preventing Prescription Opioid Diversion, American Journal of Nursing, 115(8), 34 – 40
Miller, S. (2017). A Systematic Review: The Opioid Epidemic
NASADAD, National Association of State Alcohol and Drug Abuse Directors (2018). Opioid Crisis Response Act of 2018 (S. 2680): A Section-by-Section Summary Sponsors: Senators Lamar Alexander (R-TN), Patty Murray (D-WA), Johnny Isakson (R-GA), Bill Cassidy (R-LA), Dean Heller (RNV), Joe Manchin (D-WV), Tammy Baldwin (D-WI), Tim Kaine (D-VA), Heidi Heitkamp (D-ND), Shelley Moore Capito (R-WV), Doug Jones (D- AL), Lisa Murkowski (R-AK), Orrin Hatch (R-UT), Tina Smith (D-MN), Susan Collins (R-ME), Marco Rubio (R-FL), Bob Casey (D-PA), and Claire McCaskill (D-MO) http://nasadad.org/wp-content/uploads/2018/06/The-Opioid-Crisis-Response-Act-of- 2018-5.18.18.pdf
Rutkow, L., Chang, H.Y., Daubresse, M., Webster, D.W., Stuart, E.A. and Alexander, G.C. (2015). Effect of Florida's Prescription Drug Monitoring Program and Pill Mill Laws on Opioid Prescribing and Use, JAMA Internal Medicine, 175(10): 1642-1694 doi:10.1001/jamainternmed.2015.3931



