On page 343, of your text is a question, to the left of the Euthanasia and Physician-Assisted Suicide topic (labeled: "Your Thoughts?")."Considering both courses of action will result in death, why is
Chapter 13 Dying, Death, and Bereavement

I. Death Anxiety
1. Death anxiety is common in the general public, usually higher in women, and peaks in intensity in young adulthood and declining afterward.
II. End-of-Life Decisions
A. Advance Directives
1. Advance directives refers to various types of legal documents detailing wishes of individuals regarding end-of-life concerns.
2. Advance directives, such as living wills and durable power of attorney for health care, are designed to make the wishes of an individual known when that individual is incapacitated or cannot communicate.
B. Palliative Care and Hospice Programs
1. Palliative care is focused on treating symptoms and keeping an individual comfortable (American Cancer Society, 2008; NCI, 2000).

2. Hospice care
a) A type of palliative care
C. Euthanasia and Physician-Assisted Death
1. Passive euthanasia
a) Allows “nature to take its course”
2. Active euthanasia
a) Involves taking direct action to shorten a patient’s life
b) Is illegal
3. Physician-assisted suicide
a) Could be simply responding to a patient’s questions and explaining the dosage requirements or combinations of drugs that would cause death
b) Could involve the physician actually writing the prescription for such drugs (AGS, 2005)
c) Although active euthanasia is illegal, physician-assisted suicide is legal in Oregon and in some parts of the world
III. Close to Death
A. End-of-Life Research Issues
1. End-of-life research projects face numerous challenges
a). Including convincing an IRB that the study is worth the potential Discomfort
b) Locating qualified and willing participants
B. Psychological Changes
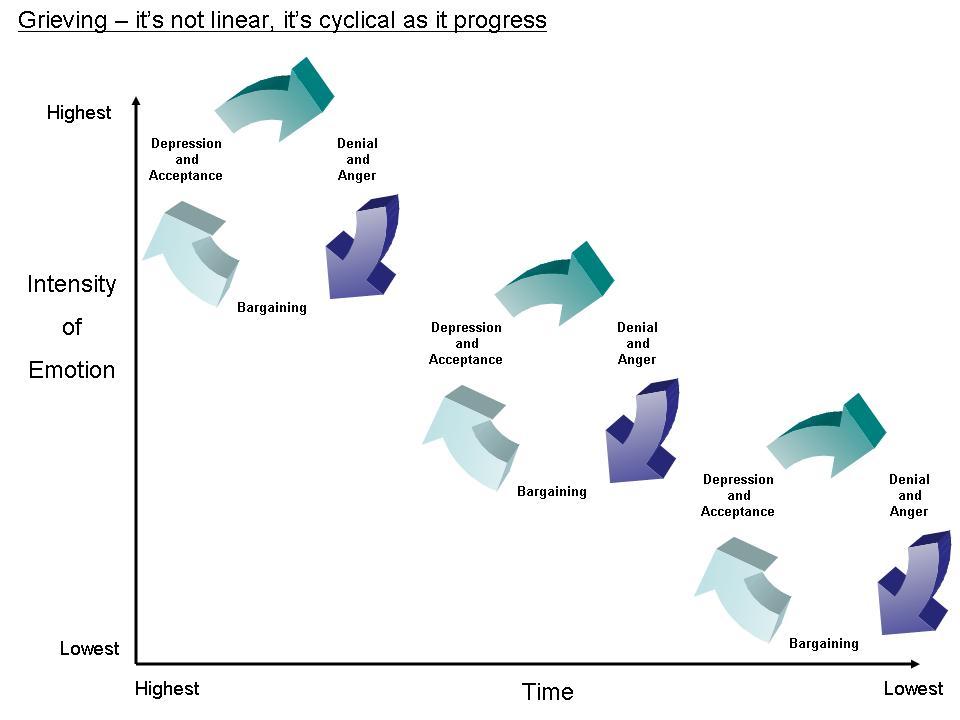
1. Kubler-Ross’ five stages of dying (denial, anger, bargaining, depression, and acceptance) was the standard portrayal of the dying experience, but it has fallen out of favor with those in the social and health sciences.
C. Interacting with Those Who are Dying
1. When interacting with someone who is dying it is important to allow honest conversation about important matters, even if it is very emotional or in some other way uncomfortable.
2. Rather than looking for an individual to follow a stage pattern, loved ones and health care professionals are encouraged to be present, listen, and be willing to engage in the difficult and emotional conversations.
D. Physiological Changes
1. As an individual approaches death, there are expected physiological signs, such as less social interaction, decrease in appetite and bladder and bowel control, cool limbs, noisy breathing, muscle contractions, and an irregular heartbeat.
IV. Transitions
A. Marking the End of Life
1. Following death, decisions need to be made regarding burial or cremation and, if desired, the type of funeral, memorial service, or public recognition of the deceased.
B. Bereavement
1. During the bereavement process individuals must learn to cope with the gap in their lives left by the deceased.


2. For most people, the symptoms of bereavement start to ease and significant healing takes place in the first 6 months.
3. Generally, individuals in bereavement pass through phases of shock, avoiding separation, disorganization and despair, and reorganization and recovery, although there may be many individual differences and circumstances that may influence one’s thoughts, behaviors, and coping skills.

C. Complicated Grief
1. Some individuals experience depression, anxiety, and prolonged and intense grieving called complicated grief.
In Assignments
Post Discussion: A few questions to ponder this week: what are your thoughts on death anxiety? Why do we distinguish between complicated grief and bereavement? What could be the impact on those individuals closest to the person experiencing complicated grief? And, on a personal level, how do you think you would respond if you discovered that someone you work closely with has a life ending situation (cancer, for example) but insists on continuing working until the last possible moment? Would you react differently if this was a family member (who wanted to continue working until the end)? These [personal] questions are not to pry but for you to have an opportunity to evaluate your own feelings on the subject.



