My paper was review by online writing service. Looking for someone to make the corrections. I will provide the paper that need changes.Hello Calvin, my name is Karen. Welcome to the Online Writing
Running head: SAFETY ISSUES IN FOOTBALL
Safety Issues in Football
Calvin C. Cunningham
Liberty University SMGT 689-01
Thesis Proposal and Research
Dr. Hatfield, Laura M
June 10, 2019
Safety Issues in Football
1.0 Introduction
Participation in physical activity is linked to multiple risks of injuries, although physical activity has many health benefits. Sports injuries are detrimental to the health of the injured athlete and may lead to permanent disability or even a termination of the sports career of the injured athlete. Injuries also present a significant burden to the healthcare system since the treatment of sport-related injuries is usually demanding and expensive (Redie, 2015). The research on injury prevention is vital to enhance the health and safety of the athletes who participate in the exercise.
Unquestionably, football is the most popular sport with an estimated population of about 265 million registered players. Football players suffer from relatively high rates of injury when compared to the participants in other types of sports. One building block of the professional sports medicine community is the prevention of injuries (Redie, 2015). Various studies have been conducted purposely to reduce ankle sprain, a common type of injury amongst the footballers. However, current research has seen an influx of projects focusing on preventing of a wide range of injuries including tendon injury, groin strains, hamstring injury, and knee injuries the anterior cruciate ligament (ACL) (Redie, 2015).
The sports prevention model follows a conceptual process that was developed by Van Mechelen. The model is a 4-step process that starts by establishing the injury prevalence, determining the mechanism of preventing each type of injury, developing and implementing prevention measures, and reevaluating the incidence of the injury to examine the success of the program (Van Beijsterveldt, 2013). In practice, there are two groups, intervention and the control group, in which the study participants are randomly assigned. The injuries sustained in the whole season are then recorded, and a comparison is made between the two groups to assess the exposure-related injury rates (Van Beijsterveldt, 2013).
Many injury preventive measures have been put in place to eradicate football-related injuries. Some of these programs include plyometric training, closed kinetic chain and strength exercises, proprioception, core stability, protective and suitable equipment, dynamic stretching, and fatigue and recovery strategies (Van Beijsterveldt, 2013). The programs have also been tailored to include appropriate training, psychology, adequate recovery, and nutrition. However, the effectiveness of these programs is based on expert opinion and logic. For instance, static stretching is widely recognized as a technique that helps in the prevention of muscle strain injuries but has been subjected to increased scrutiny of late. There is a need to establish the most efficient prevention techniques due to skyrocketing of the cases of soccer-related injuries (Van Beijsterveldt, 2013 ).
1.1 Purpose and Significance
The purpose of this research proposal is to determine the most effective interventions for preventing football injuries. The popularity of football coupled with the high demands in trailing and real match makes the players susceptible to high risk of injuries. The available evidence indicates that more than 240 million amateur and 200, 000 professional players play football. These large numbers imply that a lack of adequate and safe injury prevention programs can lead to multiple injuries among the footballers. The dangers associated with football-related injuries cannot be underestimated. Research indicates that participation in the footballing game increases the risk of traumatic brain injuries, concussions, and former players are at risk of chronic traumatic encephalopathy (CTE), a disorder which is associated with adverse effects. These injuries result in numerous debilitating effects (Tarazi et al., 2018).
Concussions occur when a ball collision hits the inside of the skull of a football player. The severity of the concussion depends on the force of the collision; a greater force of impact leads to a more severe concussion and vice versa. There are various symptoms linked to concussions, including disorientation, headaches, unconsciousness, memory problems, and fogginess (Tarazi et al., 2018). A person who had a history of concussion in the past is likely to show the symptoms of the same complication after sustaining another injury. A second concussion is always worse since its symptoms last longer when compared to the first one. CDC asserts that individuals who have suffered from two or more concussion are at higher rates of suffering from depression, personality changes, aggression, anxiety, Parkinson’s disease, Alzheimer, and CTE (Tarazi et al., 2018).
Repeated head injuries among the footballers increase the risk of CTE. The brain changes advance and become worse with time, and medical health professionals may not notice the symptoms of the disorder for several decades, years, or months after the last injury of the brain resulting in more devastating complications. Common symptoms linked to CTE include memory loss, aggression, impaired judgment, and depression (Tarazi et al., 2018). There is also evidence of the former football players with CTE who have committed murder or suicide. The condition is often diagnosed in individuals who have had repeated head injuries like former football players, boxers, and hockey players (Tarazi et al., 2018). For example, Aaron Hernadez, a former footballer who played for NFL, committed suicide while he was in prison serving time for certain murder charges. The autopsy report indicated that Hernandez was suffering from a complex CTE. Hernandez was only 27 years old at the time he was diagnosed with CTE, which was the worst to be reported on a youth. There are four phases of CTE. The fourth phase is the worst and is associated with debilitating consequences on the victim. The diagnosis report showed that Hernadez had Stage 3 of the disease, which leads to damaged thinking, behavioral changes, and memory loss (Tarazi et al., 2018).
A study conducted on deceased former footballers in 2017 established that 177 out of 202 had CTE. Players from the NFL were 111, and out of these, 110 showed evidence of CTE. However, these results do not represent all the former footballers because they only involved bodies from willing family members who donated to the study to establish the cause of death of their departed members (Tarazi et al., 2018). Although there is a wide range of reviews concerning CTE and its relationship to football players, only one case of CTE can be accurately confirmed on a former soccer player. The case involves a former NFL player known as McNeil who was subjected to an experimental brain scan in 2012. Two years after retiring, he experienced impaired movements and difficulties in executing everyday tasks like buttoning his shirt, feeding himself, and tying his shoes (Tarazi et al., 2018). The disease worsened over time, which forced healthcare professionals to refer him to a nursing home. His death came in 1963 triggering a study on his brain to establish the cause of the demise. The results came as a shock to the researchers since they recorded the symptoms that were identified in the earlier brain scans. Scientists have a passionate belief that brain scans will be applied in diagnosing CTE in living people in the future, although they are not sure whether scanning would result in any differences in the athlete’s life since the condition has no cure (Tarazi et al., 2018).
The costs of sport-related injuries among youths are substantial. Data indicates that from 2000-2003, hospital admissions for youth sports injuries cost the United States government $113 and $133 million (Tarazi et al., 2018). Therefore, more research on intervention programs for the prevention of injuries among football players is essential to maintain the player’s health, enhance his or her performance, and minimize healthcare-associated costs. Evaluating the effectiveness of injury prevention programs would enable the researchers to offer sound advice to the players, coach, team medical staff, and referees that will significantly help them in creating a conducive environment that enhances the health and safety of the footballers. The alarming rates of football injuries call for cooperation and coordination among governmental and international organizations like FIFA, FA, IOC, UEFA, and special football federations in the United States. Such information on types of prevention programs and their effectiveness would be very instrumental in guiding these organizations.
1.2 Statement of the Research Problem
Participation in physical activity increases the likelihood of injury, although physical activity has many health advantages, including lowering the rate of chronic disease development and reduction of mortality and morbidity rates. There exists a dose-response relationship between regular physical exercises and health benefits to a certain degree. Nevertheless, vigorous sports training is associated with certain disadvantages and health risks because it increases the risk of sustaining injuries. As a result, a saying has been developed that states, “injury is just part of the game.” In other words, participation in sports inevitably leads to injuries. Sports injuries have adverse effects on the health of the injured athlete and may lead to permanent disabilities or even result in termination of the career of the athlete. Injuries also present a substantial burden to the healthcare system since the treatment of sports injuries is usually expensive, time-consuming, and demanding. Therefore , there is need of research on injury prevention to promote safe practice and participation in football games by identifying the risk factors, eliminating the rates of sports injuries and maximizing the health advantages gained in being part of the game.
Some of the research questions that guide this study include:
What model provides guidelines for implementation of techniques for preventing sport-related injuries?
What are the risk factors that predispose soccer players to injuries?
What are some of the evidence-based methods for preventing sport-related injuries?
2.0 Literature Review
2.1 The Sequence of Prevention Model
The “sequence of prevention” model was published by Van Mechelen et al. in 1992 to analyze the growing problem of sport-related injuries (Van Beijsterveldt, 2013). The four-step model comprehensively describes how one should ideally perform epidemiological research on sports injury (Figure 1). Step 1 involves identification of the magnitude of the soccer-related injury challenge and elucidating it using the severity and prevalence terms. Phase 2 entails identification of the mechanisms and factors that contributes to the cause of sports injuries (Van Beijsterveldt, 2013). Step 3 introduces measures that significantly help in reducing future severities and risks of sports injuries. The standard adopted in this step is often based on the mechanisms and etiological factors identified in the second step. Step 4 is the final phase and includes evaluating the measures by repeating the first step (Van Beijsterveldt, 2013).
Step 2: Establishing the etiology and mechanisms of sports injuries

Step 1: Establishing the extent of the Injury Problem: injury and severity


Step 4: Assessing its effectiveness by repeating step 1
Step 3: Introducing a preventive measure

Figure 1: Sequence of Prevention: the four-step model of sports injury research.
Several studies have been conducted on the prevention of soccer-related injuries due to the prevalence rates of the injuries, the pain and trauma suffered by the players, and the medication costs linked to the injuries (Van Beijsterveldt, 2013). Up to date, it is only shin guard that has been made mandatory to be won during football matches to prevent shinbone fractures. Thirty-three studies which examine injury preventive techniques for football players have been conducted in line with step 3 of the sequence prevention (Van Beijsterveldt, 2013). These studies have established several interventions for preventing soccer-related injuries. Some of these measures include orthoses, balance training, video-based awareness, strength training, and multi-component training programs (Van Beijsterveldt, 2013). The participants of 17 of these studies comprised of male footballers, 13 consisted of female players, and the remaining three studies examined mixed cohorts. Twenty-six out of these 33 studies found that soccer injury prevention measures lead to a reduction in primary or secondary outcomes. Examples of these outcomes include acute injuries, injuries overall, repetitive injuries, and injuries to parts of the human body, such as hamstring strain, ankle sprain, and anterior cruciate ligament injuries (Van Beijsterveldt, 2013).
Sixteen studies examined the impact of applying an intervention to one specific injured part with different studies evaluating ankle, hamstring, knee, and groin injuries in their sample populations. The findings of the reviews indicated that ankle braces are a useful technique for reducing the recurring ankle sprains in both women and men footballers. Furthermore, balance training was found to be instrumental in reducing the risk of recurrent or new ankle sprains in youth soccer players and adult male and female players (Van Beijsterveldt, 2013). However, the findings of intervention studies concentrating on knee injuries in different sample populations are ambiguous. Some studies documented results of preventive effects, whereas others established that these interventions do not lead to a reduction of the primary outcomes. Finally, the available literature indicates that multi-component programs are fundamental in preventing overall football-related injuries, mostly in female youth players (Van Beijsterveldt, 2013). The programs are often conducted during the warm-up of soccer training and comprise a combination of exercises which substantially aid in improving balance, coordination, strength, and agility. However, the efficacy of such techniques is yet to be proven for the most significant and dominant force in football; adult male footballers (Van Beijsterveldt, 2013).
2.2 Risk Factors
By observing casually, one might think that soccer injuries are random accidental events. However, the fact remains that there are various factors which play a significant role in the cause of musculoskeletal injuries. Multiple studies have agreed that sport-related injuries occur due to the complex interaction of numerous events and risk factors. In the literature, these risk factors are categorized into two main classes: intrinsic and extrinsic elements (Leppänen, 2013). Intrinsic factors refer to the factors that increase the risk of sustaining injury and predispose the footballer to injury. Extrinsic factors relate to the factors that modify the risks by increasing the vulnerability of the footballer to the injury (Leppänen, 2013). Both risk factors make a player susceptible to fractures. An exciting event (like a fall or a tackle) which is often related to the injury completes the chain. It is essential to consider all the elements of the chain to gain a comprehensive understanding of the whole picture (Leppänen, 2013). An analysis of the multifactorial model of athletic injury etiology developed by Meeuwise helps us in understanding the entire image, as shown in Figure 2 below:
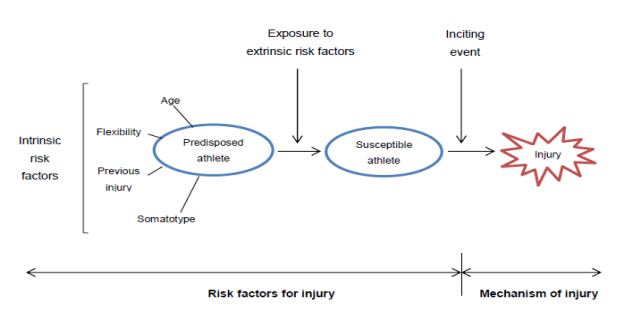
Figure 2: Relationship between intrinsic and extrinsic factors and soccer injury.
2.2.1 Intrinsic factors
Intrinsic factors refer to individual psychosocial and physical characteristics that predispose a footballer to musculoskeletal injury outcomes. These factors include age, body composition, physical fitness, gender, health, injuries, anatomy, sports-specific skills, and abilities. According to the findings of numerous studies, age increases the risk of sustaining soccer-related injuries (Leppänen, 2013). The coaching programs for professional football players are characterized by increased intensity and frequency, which increases the likelihood of sustaining a musculoskeletal injury compared to amateur players. Sports participation presents one of the most substantial risk factors that increase hospitalization rates in early adulthood and adolescent players (Leppänen, 2013 ).
Men recorded higher rates of injury during the 2000 Olympic Games and the 1998 men’s World Cup when compared to women during the 2000 Olympic Games and 1999 Women’s World Cup. However, no difference was recorded in both men and women during the 2004 Olympics and the men and women’s European championships that took place in 2004 and 2005 respectively (Leppänen, 2013). Two studies examined the prevalence of injury during indoor tournaments and recorded no differences in the overall rates of injury between men and women (Leppänen, 2013). Studies indicate that ACL injury risk among the female footballers is higher when compared to the male footballers, and the female football players also sustain these injuries at a younger age compared to the male soccer players. The rates of concussions, on the other age , is higher in male footballers than the women footballers (Leppänen, 2013).
Anthropometrics, physical abilities, and anatomical factors play a pivotal role in influencing the risk of soccer-related injuries. Increased weight and body mass index (BMI) predispose players to ankle joint injuries (Leppänen, 2013). Moreover, asymmetries like eccentric muscle strength of the lower extremity and the functional length leg increase the risk of sustaining leg injuries. Besides, neuromuscular deficiencies including delayed muscle firing, muscle weaknesses, and defective muscle activations are linked to increased risks of injuries. The level of aerobic fitness is also instrumental in determining the risk of injury since fatigue lowers muscle control and coordination (Leppänen, 2013).
2.2.2 Extrinsic Factors
Intrinsic factors are linked to the type of activity under progress and do not depend on the injured footballer. These factors are categorized into training, environment, exposure, and equipment. The exposure factors include the type of sporting activity, time of exposure, level of competition, and position of the player in the team (Leppänen, 2013). A range of elements such as type, frequency, amount, and training intensity comprise of the training factors of which specific training errors like immediate initiation of training plays an enormous role in the injury outcome. There are various equipment factors which substantially influences the risk of injury, including sports equipment (e.g., clothing, racket, footwear, and skis) and protective devices (e.g., shin guards and helmets). Environmental risk factors include the playing ground or surface, time of the season, the condition of the weather, indoor and outdoor conditions together with human factors like coaching, referees, opponents, rules, teammates, and spectators (Leppänen, 2013).
2.3 Injury Prevention Programs
2.3.1 Plyometric Programs
Determination of injury predispositions enables the medical team and sports scientists to target these areas of weaknesses in footballers that helps in limiting the possibility of sustaining an injury (Reddie, 2015). The ratio of hamstrings to quadriceps and the muscle strength of the dominant and non-dominant hamstring are some of the most significant indicators of injury predispositions. Certain factors, such as the amount of force absorbed upon landing, functional biomechanics, and active joint stabilization, play an enormous role in causing an ACL injury (Reddie, 2015). Plyometric training and strength interventions aim at improving the capacity of the football player in the areas mentioned above by incorporating exercise programs that increase power, speed, agility, and strength. In so doing, female footballers who exhibit these powerful features can increase their sub-standard baseline strengths to match the level of the male soccer players. Research indicates no statistical differences exists between the ratio of hamstring to quadriceps between female and male footballers after the implementation of strength and plyometric training (Reddie, 2015). Therefore, female footballers experience decreased ‘quad dominance’ that reduces leg hyperextension risk and subsequent attack by ACL strain and other types of injuries.
Plyometric training comprises of jumping and hopping exercises coupled with ballistic movements that contain both eccentric and concentric phases. The purpose of a plyometric training program is to enhance the movement of the biomechanics in the soccer players and to reduce eccentric contraction conversion to a concentric contraction in muscles, and the process help in the release of the stored energy (Reddie, 2015). Specifically tailored female players plyometric programs are developed to bring neuromuscular adaptation to the musculature around the knee, to lower Varus and Valgus torques that cause knee injuries and the ACL (Reddie, 2015).
2.3.2 Proprioceptive Training
Proprioception is a unique variation of the sensory modality of touch that involves the sensation of joint position sense and joint movement (kinesthesia). Knowing the location of limb spatial awareness and location of limbs in the space is one of the most important things to the footballers (Reddie, 2015). Female football players need to increase the spatial awareness by allowing more centeredness and ridging of the core during the act of jumping and enable plantation of the limbs in safe locations that maximize the protection against injury. The available evidence indicates that disruptions to somebody structures like the ACL leads to impairments of the articular structures that contain mechanoreceptors (Reddie, 2015). This leads to loss of the capability of kinesthesia and certain joint position sense because of the decreased limb proprioception that plays an instrumental role in re-injuring a soccer player. As a result, proprioceptive training of soccer players is crucial to rehabilitation and injury pre-habilitation. A study has established that football players with proprioceptive deficits are likely to suffer from injuries. Female have poor knee proprioception since they have deficiencies in hamstring with slow forces and reaction times (Reddie, 2015). As a consequence, increasing the readiness of the muscle spindles, rates of muscle firing, and mass of the muscles in the hamstring area of the female footballer who is undertaking a cutting movement or trying to land from a jump does so with increased dynamic knee stability, therefore reducing the chances of an injury (Reddie, 2015).
2.3.3 Closed Kinetic Chain and Strength Exercises
History of previous injuries is one of the primary predisposing factors to injuries among the soccer players (Reddie, 2015). Closed kinetic chain exercises have proved pivotal in rehabilitating ACL injury footballers, and these exercises are more preferred to open chain kinetic exercises because of their ability to accelerate rehabilitation from injuries and safeguards further injuries to the injured joints and tissues of the soccer player. Closed chain exercises entail both ends of joints that are fixed (Reddie, 2015). Although this cannot be applicable in a real sense since the acetabulum of the pelvis is joined to the proximal head of the femur, weight-bearing exercises that aim at improving the stability of the knee where the feet are on the ground are regarded as closed chain exercises. Examples of exercises in this category include deadlifts and squats and are highly recommended to uninjured players since they improve the strength of musculature around the knee and increases muscle mass thus enhancing the stability and strength of these footballers (Reddie, 2015). Closed chain exercises have been found useful in improving the strength of players with weak ACLs. The compression of the joints during the closed kinetic chain exercises leads to an increase in joint stability. There are various reasons why female footballers should perform resistance strength exercises. Evidence indicates that resistance training provides performance gains and injury prevention advantages when combined with other techniques such as plyometric work and proprioception. A combination of resistance training with proprioception and plyometric work gives the footballer explosive power around controlled ranges of motion (Reddie, 2015).
2.3.4 Strength and Resistance Exercise
An excessive anterior translation occurs during dynamic activities when the quadriceps are stronger than the hamstrings, which forces ACL to experience shear forces. Therefore, balancing the strength of the hamstring to that of the quadriceps is vital since it maintains a right hamstring: quadriceps ratio. Research shows that plyometric training improves the H: Q ratio (Reddie, 2015). Resistance training significantly helps in supplementing plyometric training hence further enhancing the strength of the hamstring. Exercises like deadlifts and squatting improve leg musculature but do not influence the ratio of hamstring to quadriceps despite the fact it makes the footballer stronger (Reddie, 2015). We can be able to apply injury prevention interventions such as resistance exercises to increase the strength of the hamstring, and thus reduce the ACL strain if only we understand that hamstring muscles are located on ACL agonist and resist forces that strain the ACL. Specific exercises that target the hamstrings are recommended since they decrease the muscle imbalances (Reddie, 2015). An excellent example of such a practice is the Assisted Russian Hamstring Curls or Nordic Hamstring Curls. In the Nordic Hamstring Curls, the ankle of a footballer is strapped down by his or her training partner in this exercise, and the player is advised to eccentrically lower himself forward, maintaining his core tensed and rigid. The soccer player is expected to lower his upper body towards the ground and oppose his body weight and gravity, until the climax stage where he can no longer do so. In the Assisted Russian Hamstring Curls, the player is aided in lifting herself back to the starting position by utilizing a resistance band which is tied around her waist (Reddie, 2015).
3.0 Methodology
The randomized controlled trial (RCT) will aim at evaluating the efficacy of injury prevention interventions by inviting teams in the English Premier League to participate in the study. The fact that the survey will apply RCT design implies that it is a quantitative research approach. The ethical approval to conduct the research will be sought from the ethics committee of the University of Boulevard, Lynchburg, Virginia. Both male and female players between 18-40 years will be eligible for inclusion. The players included in the study must have at least three to four practice sessions per week. A form of informed consent will be signed by all the players before the start of the study. The injury prevention programs will be developed with the support of the World Football Association FIFA. Ten exercises will be designed focusing on eccentric training, plyometric training, proprioceptive training, and dynamic stabilization. The coaches in the intervention group will be advised to integrate these techniques during the 2019/2020 soccer season. The coaches will be trained on how to apply for the injury prevention programs in July 2019 before the start of the new season. Besides, these coaches will receive a detailed information package consisting of a DVD, reader, and poster that will contain the basic elements of the injury prevention interventions. The coaches in the intervention group will be required to familiarize themselves with the program during the four weeks on August preceding the start of the season. The coaches in the control group will be invited in a study of the injury incidence and characteristics of practice. The date will be recorded, and the SPSS 17 will be used to perform analyze the data.
References
Leppänen, M. (2013). Prevention of sports injuries: systematic review and meta-analysis of randomized controlled trials.
Reddie, C. L. (2015). What Can an Athlete Do to Reduce the Risk of Injury?
Tarazi, A., Tator, C. H., Wennberg, R., Ebraheem, A., Green, R. E., Collela, B., ... & Tartaglia, M. C. (2018). Motor function in former professional football players with history of multiple concussions. Journal of neurotrauma, 35(8), 1003-1007.
Van Beijsterveldt, A. M. C. (2013). Injury prevention for adult male soccer players. Utrecht University.



