Program Outcome 4 Please respond to the following discussion topic and submit to the discussion forum as a single post. Your initial post should be a minimum of 150 words in length. Then, make at leas
CHAPTER 4
Leadership and the Manager
CHAPTER OBJECTIVES
• Address the role of the manager as a principal agent of change.
• Differentiate among the terms power, influence, and authority.
• Recognize the importance of authority for organizational stability.
• Identify the sources of power, influence, and authority.
• Relate the sources of power, influence, and authority to the organizational position of the line manager.
• Recognize the limits placed on the use of power and authority in organizational settings.
• Recognize the importance of delegation of authority.
• Explore the nature of leadership and the reasons why individuals seek leadership positions.
• Identify the styles of leadership, their characteristics, and the circumstances under which they are applied.
CHANGE AND THE MANAGER
The healthcare setting of today is a highly dynamic environment in which the individual manager must embrace the reality of constant change and accept and fulfill the role of change agent within the organization. It is only through addressing essential change and truly leading employees in its acceptance and implementation that the manager can be successful in the long term. Denying or resisting change does not merely mean standing still but losing ground and actually going backward relative to technology and society as they race ahead.
The department manager must be able to deal with employee resistance to change, including the most frequently encountered causes of resistance and how best to approach resistance to change with employees. However, this implies that the manager is already completely on board with the necessity for a particular change. It is now appropriate to acknowledge that the manager may well be fully as susceptible to resistance as the employees. Who is the manger but simply another employee? He or she can be just as affected by misgivings and uncertainty about impending change as the rank-and-file staff. A discussion of how managers may deal with change appears in Chapter 2.
Thus, the manager may have a difficult task up front in the implementation of change, especially change mandated “from on high” or forced by external circumstances, because the manager has nearly the same potential for resistance as the employees. Even the knowledge that a certain change is inevitable regardless of what it entails does not necessarily guarantee that the manager will be a willing advocate for the change.
Of course the manager, and just about everyone else for that matter, is likely to champion a change that was his or her own idea. But when ideas or directives or other requirements come from elsewhere, the manager, who may experience some feeling of resistance, must deliberately strive to overcome that feeling and become champion of the change. It is often extremely difficult for the manager who feels some personal misgivings to go forward as the driver of change.
We are told repeatedly that the manager can address change with the employees in three ways: tell them what to do, convince them of what must be done, or involve them in determining what must be done. This third approach, involving them, is all well and good—but often it cannot be used. The first approach, the tell-them-what-to-do route, is avoided if possible because it does little to temper resistance. This leaves the second approach, the need for the manager to convince the employees of what must be done. Clearly, many employees are more likely to get on board with a particular change if they know why it must be done. And an honest why is not simply telling the employees that it is “orders from administration” or blaming it on the ever-present yet never identifiable “they” as in “they are making me do it.”
The central point of this brief discussion is that if the manager is to be a true agent of change and an honest and effective catalyst for change, the first person to be accepting and supportive of change is the manager. So if you, the manager, experience doubts or misgivings about some change that lies ahead, work these out within yourself and with your superiors as necessary. Your employees should be able to see you as a true agent of change who is there to support their efforts in implementing change and helping them through it such that everyone, yourself included, achieves a new comfort zone as essential change becomes part of the norm.
WHY FOLLOW THE MANAGER?
The manager issues an order or directive, and the result is compliance. But why do employees obey? Is it even appropriate to use the term obey to describe this compliance? Which bases of authority are operative in superior–subordinate transactions? What are the limits of a manager’s authority? What if a particular supervisor is seen as a weak manager? Are there remedies available for addressing problems related to weak or ineffective management leadership? Of what value to the organization is the authority structure? What are the consequences for life within the organization if there is not general, unchallenged compliance most of the time? When actions of compliance are described, which term provides the proper point of reference—power, authority, or influence? Are these terms mutually exclusive or are they synonymous when used in the context of organizational relationships? These questions arise when discussion of authority in organizations is undertaken.
Organizational behavior is controlled behavior, behavior that is directed toward goal attainment. The authority structure is created to ensure adherence to organizational norms, to suppress spontaneous or random behavior, and to induce purposeful behavior consistent with the aims of the organization. No matter how the work within the organization is divided, no matter the extent to which specialization, departmentation, centralization, or decentralization is formalized, there must be some measure of legitimate authority if the organization is to be effective. The concept of formal authority is supported by the two related concepts of power and influence. These concepts may be separated for analytical purposes; in actual practice, however, the concepts of authority, power, and influence are intertwined.
THE CONCEPT OF POWER
Power is the ability to obtain compliance by means of some form of coercion, whether blatant or subtle; one’s own will prevail even in the face of resistance. Power is force or naked strength; it is a mental hold over another. Like authority and influence, power is aimed at encouraging compliance, but it does not seek consensus or agreement as a condition of that compliance.
Power is always relational. An individual who has power over another person can narrow that person’s range of choices and obtain compliance. The power holder does not necessarily force compliance by physical acts but rather may operate in more subtle ways, such as an implied threat to apply sanctions. Latent power is frequently as effective as an overt show of power. Power attaches to people, not to official positions. The formal authority holder (i.e., the person who has the official title, organizational position, and grant of authority) may or may not have power in addition to this formal grant of authority.
An imbalance in superior–subordinate relationships can occur when a nonofficeholder has more power than the official officeholder. This can even be seen in family life. For example, when a 2-year-old boy shows signs of an incipient temper tantrum in the middle of the annual family gathering, the power balance clearly is in favor of the child if the tantrum pattern has developed. The child does not have to carry out the explosive behavior; the mere threat of the possibility brings about some desired behavior from the parent caught in the situation.
Workers often have some degree of power over line supervisors and managers. A worker with specific technical knowledge can withhold key information from a manager or can develop a relationship that is personally favorable. Information may not actually be withheld; the mere possibility that the manager cannot rely on an individual is enough to shift the balance, at least temporarily, in favor of the worker. Groups of workers can control a manager when it is known that the manager is responsible for meeting a deadline or filling a quota; the manager’s ability to do so is dependent on the cooperation of the workers. Normal, steady output may be produced routinely, but the ability to make that extra push needed to surpass the quota or reach a special level of output rests more with the workers than with the manager. Strikes by workers are classic examples of mobilized power, but the power shifts back in favor of management if striking workers are terminated during a strike.
When an individual can supply something that a person values and cannot obtain elsewhere in an accepted manner, or when the individual can deprive one of something valued, then there is a power relationship. This implicit or explicit power relationship may or may not be perceived by one or both parties.
THE CONCEPT OF INFLUENCE
Like power, influence is the capacity to produce effects on others or obtain compliance from others, but it differs from power in the manner in which compliance is evoked. Power is coercive, but influence is accepted voluntarily. Influence is the capacity to obtain compliance without relying on formal actions, rules, or force. In relationships governed by influence, not only compliance but also consensus and agreement are sought; persuasion rather than latent or overt force is the major factor in influence. Influence supplements power, and it is sometimes difficult to distinguish latent power from influence in a given situation. Does the individual comply because of a relationship of influence or because of the latent power factor? Together, power and influence supplement formal authority.
THE CONCEPT OF FORMAL AUTHORITY
Authority may be described as legitimate power. It is the right to issue orders, to direct action, and to command or exact compliance. It is the right given to a manager to employ resources, make commitments, and exercise control. By a grant of formal authority, the manager is entitled, empowered, and authorized to act; thus, the manager incurs a responsibility to act. Authority may be expressed by direct command or instruction or, more commonly, by request or suggestion. Through the delegation of authority, coordination is established in the organization.
The authority mandate is delineated, communicated, and reinforced in several ways, including organizational charts, job descriptions, procedure manuals, and work rules. Although the exercise of authority in many situations tends to be similar to transactions of influence, authority differs from influence in that authority is clearly vested in the formal chain of command. Individuals are given specific grants of authority as a result of organizational position. Power and influence may be exercised by an individual authority holder, but they may also be exercised by individuals who do not have specific grants of authority.
Authority is both complemented and supplemented by power on the one hand and influence on the other hand. It is within the realm of formal authority to exact compliance by the threat of firing a person for failure to comply; however, this may be such a rare occurrence in an organization that such a threat is really an application of power more than an exercise of authority. However, formal aspects of authority may be so well developed that the major transactions remain at the level of influence, with the influence based largely on the holding of formal office. The infrequent use of formal authoritative directives to evoke compliance may indicate organizational health; that is, people know what to do and perform willingly.
THE IMPORTANCE OF AUTHORITY
When a subordinate refuses to accept the orders of a superior, the superior has several choices, each of which carries potentially negative consequences for the attainment of organizational goals. The superior can accept the insubordination, withdraw the order, and call on others to carry out the directive. This action would probably further weaken authority, however, because the superior would most likely be perceived as lacking the subtle blend of power and authority needed to exact compliance on a predictable basis. A chain reaction of insubordination could occur. If other workers are asked to carry out a directive that had been refused by one worker, resentment could build up and produce negative consequences. If the order is withdrawn completely, of course, the work will not be accomplished.
The manager who decides to enforce compliance may suspend or fire the insubordinate worker, but the superior still must find a worker to carry out the directive. If there is a chain reaction of insubordination, it may become impractical to suspend or fire the entire work force. In such circumstances, the situation moves from one of authority to one of power. Therefore, managers must identify and widen their bases of authority to help ensure a stable work climate.
SOURCES OF POWER, INFLUENCE, AND AUTHORITY
The manager’s organizational relationships flow along the continuum of power, influence, and authority, varying in emphasis at different times and in different situations. To more fully understand the dynamics of the power–influence–authority triad, it is useful to examine the sources or bases of authority in formal organizations. The wider the base of authority, the stronger the manager’s position; with a broad base of authority, the manager can work in the realm of influence and need not rely only on the formal grant of authority that attaches to organizational position.
The sources of formal authority have been studied by several theorists in the disciplines of social psychology, management, and political science. A review of the literature suggests several sources or bases of authority: (1) acceptance or consent, (2) patterns of formal organization, (3) cultural expectations, (4) technical competence and expertise, and (5) characteristics of authority holders. The limits or weaknesses of each theory are offset by the approach taken in another.
The Consent Theory of Authority
The belief that authority involves a subordinate’s acceptance of a superior’s decision is the basis for the acceptance or consent theory of formal authority. A superior has authority only insofar as the subordinate accepts it. This theory implies that members of the organization have a choice concerning compliance, even when often they do not. It remains important to recognize the concepts of acceptance and consent to identify the centers of more subtle and diffuse resistance to authority, even when there is no overt and massive insubordination.
The zone of indifference and the zone of acceptance are two similar concepts in the acceptance or consent theory of authority. Chester Barnard used the term zone of indifference to describe that area in which an individual accepts an order without conscious questioning.1 Barnard noted that the manager establishes an overall setting by means of preliminary education, prior persuasive efforts, and known inducements for compliance. The order then lies within the range that is more or less anticipated by the subordinate, who accepts it without conscious questioning or resistance because it is consistent with the overall organizational framework. Herbert Simon used the term zone of acceptance to reflect the same authority relationship. The zone of acceptance, according to Simon, is an area established by subordinates within which they are willing to accept the decisions made for them by their superior.2 Simon noted that this zone is modified by positive and negative sanctions in the authority relationship, as well as by such factors as community of purpose, habit, and leadership.
Coupled with the foregoing factors is the concept of the rule of anticipated reactions, which Simon included in his discussion of the zone of acceptance.3 According to this rule, subordinates seek to act in a manner that is acceptable to their superior, even when there has been no explicit command. The authority system, including anticipated review of actions, is so well developed that the superior needs only to review actions rather than issue commands. The past organizational history in which positive and negative sanctions were enforced is recalled; the expectation of the review of actions is fostered so that the subordinates’ zone of acceptance is expanded.
Another approach to the concept of authority as a relationship between organizational leaders and their followers is described by Robert Presthus, who posited a transactional view of authority in which there is reciprocity among individuals at different levels in the hierarchy.4 Compliance with authority is in some way rewarding to the individual, and the individual, therefore, plays an active role in defining and accepting authority. Everyone has formal authority, in that each person has a formal role in the organization. There is, Presthus stated, an implicit bargaining and exchange of authority, with each individual deferring to the other.
The notion of reciprocal expectations in authority relationships is further supported in Edgar Schein’s discussion of the psychological contract.5 As in Barnard’s concept of the zone of indifference and in Simon’s rule of anticipated reactions, the premise of member acceptance of organizational authority and its attendant control system is basic to the psychological contract. The workers’ acceptance of authority constitutes a realm of upward influence; in turn, the workers expect the authority holders to honor the implicit restrictions on their grant of authority. The workers expect the authority holders to refrain from ordering actions that are inconsistent with the general climate of the given organization and from taking advantage of the workers’ acceptance of authority. The workers also expect as part of this psychological contract the rewards of compliance (i.e., positive sanctions readily given and negative sanctions kept at a minimum).
The Theory of Formal Organizational Authority
In his classic study of bureaucracies, Max Weber discussed three forms of authority: charismatic, traditional, and rational–legal. Charisma, as defined by Weber, is a “certain quality of an individual personality by virtue of which he is set apart from ordinary men and treated as endowed with supernatural, superhuman, or at least specifically exceptional qualities.”6 The social, religious, and political groups that form around charismatic leaders tend to lack formal role structure. The routines of bureaucratic structure are not developed and may even be disdained by the group. Charismatic authority figures function as revolutionary forces against established systems of leadership and authority. Such authority is not bound by explicit rules but rather remains invested in the key charismatic individual. Personal devotion to the leader or what might be termed an almost irrational faith in the leader bind the members of the group to one another and to the leader.
Because charismatic authority is linked to the individual leader, the organization’s survival is similarly linked. If the organization is to endure, it must take on some of the characteristics of formal organizations, including a formalized authority pattern. In this area, two developments are possible. Charismatic leadership may evolve into a traditional system of authority, or it may develop into the rational–legal system of formal authority. In traditionalism, a pattern of succession is developed. A successor may be designated by the leader or hereditary/kinship succession may be established; then a system of transferring the leadership to the legitimately designated individual or heir must be developed. This, in turn, leads to a system of roles and formal authority. Weber uses the term routinization of charisma to describe this transformation of charismatic authority into, first, traditional authority, and then rational–legal authority.
Rational–legal authority is the authority predicated in formal organizations. It is generally assumed that formal organizations come into being and derive legitimacy from an overall social and legal system. Individuals accept authority within the formal organizational structure because the rights and duties of members of the organization are consistent with the more abstract rules that individuals in the larger society accept as legitimate and rational.
Within the formal organization, a system of roles and authority relationships is carefully constructed to enable the organization to survive and move toward its formal goal on a continuing, stable basis. Authority has its basis in the organizational position, not in any individual. Weber described in detail the major characteristics of bureaucratic structures; the following characteristics relate to the rational-legal authority structure:7
1. The principle of fixed and official jurisdictional areas means that areas are generally ordered by rules—that is, by laws or administrative regulations.
a. The regular activities required for the purposes of the bureaucratically governed structure are distributed in a fixed way as official duties.
b. The authority to give the commands required for the discharge of these duties is distributed in a stable way and is strictly delimited in a fixed way as official duties.
c. Methodical provision is made for the regular and continuous fulfillment of these duties and for the execution of the corresponding rights; only persons who have generally regulated qualifications to serve are employed.
2. The principles of office hierarchy and of levels of graded authority mean that there is a firmly ordered system of superiority and subordination in which supervision of the lower offices is carried out by the higher ones.
The theory of formal organizational authority rests on this rational–legal system of formal office, impersonality of the officeholder, and a system of rules and regulations to constrain the grant of authority. Delegation of formal authority from top management to each successive level of management is the basis of formal organizational authority. Authority is derived from official position and is circumscribed by the limits imposed by the hierarchical order.
Cultural Expectations
Both the consent theory of authority and the theory of formal organizational authority include an implicit assumption that individuals in a society are culturally induced to accept authority. Furthermore, the acceptable use of authority in organizations is defined in part by the larger societal mores as well as by union contract, corporate law, and state and federal law and regulation.
Acceptance of the status system in a society is learned as part of the general socialization process. General deference to authority is ingrained early in psychosocial development, and social roles with their sanctions are accepted and reinforced throughout life. The role of employee carries with it both formal and informal sanctions; insubordination is not generally condoned. Even as a group cheers the occasional rebel, there is attendant discomfort because something is out of order in the relationship. When the insubordination of an individual begins to threaten the economic security of the group, there is counterpressure on that individual to bring about reacceptance of authority. Fear of authority may bring about a similar response of renewed acceptance of authority and counterpressure on any dissidents.
The expected zone of acceptance or zone of indifference varies with different social roles. These variables are rarely spelled out in great detail; they are learned as much through the pervasive cultural formation process as through the formal orientation process in any one organization. There is a kind of “group mind” that includes the general realization that a particular behavior pattern is part of a given role, and the entire role set reinforces this general acceptance of authority.
Technical Competence and Expertise
Three terms reflect the organizational authority that is derived from or based on the technical competence and expertise of the individual, regardless of which office or position the individual holds in the organization. These terms are functional authority, law of the situation, and authority of facts.
Functional authority is the limited right that line or staff members (or departments) may exercise over specified activities for which they are responsible. Functional authority is given to the line or staff member as an exception to the principle of unity of command. For purposes of this discussion on the sources of authority, it is useful to emphasize the special character of functional authority, which is given to a line or staff member primarily because that individual has specialized knowledge and technical competence. For example, the human resources manager normally assists all other department heads in matters of employee relations, although this manager has no authority to intervene directly in manager–employee relations. The situation changes when there is a legally binding collective bargaining agreement: the human resources manager, with special training in labor relations, may be given functional authority over all matters stemming from the union contract because of specialized knowledge. Another example is that of information technology support staff who, because of technical competence, are given authority to make final decisions over certain aspects of data collection. The authority is granted because of the technical competence of the staff members.
Mary Parker Follett, a pioneer in management thought, introduced the terms law of the situation and authority of facts.8 Follett described the ideal authority relationship as that stemming from the situation as a whole. Each participant in the organization who is assumed to have the necessary qualifications for the position held has authority associated with that position. Orders become depersonalized in that each participant in the process studies and accepts the factors in the situation as a whole. Follett stated that one person should not give orders to another person but rather both should agree to take their orders from the situation.9 She developed this concept further: both the employer and the employee should study the situation and should apply their specialized knowledge and technical competence through the principles of scientific management. The emphasis shifts, in Follett’s approach, from authority derived from one’s official position or office to authority derived from the situation. The individual who has the most knowledge and competence to make the decision and issue the order in a particular situation has the authority to do so. The staff assistant or a key employee potentially has as much authority in a particular situation as does the holder of a hierarchical office. The incident command system used in hospital disaster management is an example of law of the situation, with command passing from unit manager, clinical specialist, or safety officer as the circumstance requires.
Closely tied to the concept of law of the situation is that of authority of facts. Follett stressed that, in modern organizations, individuals exercise authority and leadership because of their expert knowledge.10 Again, leadership and authority shift from the hierarchical position to the situation. The person with the knowledge demanded by the situation tends to exercise effective authority.
Both of these concepts place emphasis on the depersonalization of orders. At the same time, the source of the authority is highly personal, in that knowledge and competence for the exercise of authority belong to an individual. Underlying the concepts of functional authority, law of the situation, and authority of facts is the theme that authority is derived from the technical competence and knowledge of individuals in the organization who do not necessarily hold formal office in the line hierarchy.
Characteristics of Authority Holders
Authority rests in individuals. The talents and traits of the individual may become the source of authority, as in the case of the charismatic leader. A person holding power may use this as a base for gaining legitimate authority, or a group may invest the person of power with legitimate authority as a protective measure and seek to impose the limits and customs of authority. They may also accept the power holder as formal officeholder as a means of accepting the situation without further conflict. Technical competence and knowledge are also personal characteristics that become the basis of authority in certain situations.
Authority by Default
A weak form of authority stems from situations in which the group members, either by conscious decision or by lack of attention to authority–leadership succession, do not develop strong, clear, authority patterns. A professional organization, for example, might decide to rotate authority–leadership roles through a nomination process that limits the choice of candidates from specific geographic regions. In another organization, the committee chair role might be simply rotated through all the members in turn, either because members do not wish to have any one department as dominant or simply because the task is seen as a chore. In another organization, provision for succession might be weakened because the same few members hold officer positions for years, so no new leadership is developed.
Of course, the time invariably comes when a long-term authority holder is no longer able to continue. A vacuum then arises, and a newer member is prevailed on to assume the office. When such occurs, authority by default is the rule. The officeholder must attend to building up the office or accept the realities of the situation, as he or she has only a limited authority mandate.
The Manager’s Use of Sources of Authority
In practice, managers should recognize all the potential sources of authority and weigh the contribution of each theory to obtain as complete a picture of the authority nexus as possible. They should assess their own grants of authority and try to determine which elements tend to strengthen their authority and which tend to erode it.
The base of authority shifts from time to time. As an example, suppose an individual is offered the position of department head of a health information service because of that individual’s competence in the administration of health information systems; this specialized knowledge and technical competence is the first pillar of authority. When the individual accepts the position, the formal authority mandate of that official position is added. This authority, in turn, is shaped by the prevailing organizational climate, which includes either a wide or narrow zone of acceptance on the part of employees. The personal traits of the authority holder complete the authority base for that office.
The individual with a participative management style may emphasize those aspects of authority that widen the zone of acceptance. The setting itself may dictate the predominant authority base, as in the law of the situation; in a highly technical setting, those persons with the most technical knowledge use this knowledge as the base of authority. Although there is a tendency to downplay internal politics in organizations such as healthcare institutions, some individual managers may use power as a major source of authority. Astute managers regularly assess the several bases of authority available to them to enhance the authority relationships and thereby contribute more effectively to the achievement of organizational goals.
RESTRICTIONS ON THE USE OF AUTHORITY
Several factors restrict the use of authority. Some constraints stem from internal factors, such as the limits placed on authority at each organizational level; others stem from external factors, such as laws, regulations, and ethical considerations. The following is a systematic summary of these factors:
1. Organizational position. Each holder of authority receives a limited delegation of authority consistent with the position held in the organization. An individual has no legitimate formal authority beyond that accorded to the organizational position.
2. Legal and contractual mandates. Authority is limited by federal, state, and municipal laws and regulations relating to safety, work hours, licensure, and scope of practice; by internal corporate charter and bylaws; and by union contract.
3. Social limitations. The social codes, mores, and values of society at large include both implicit and explicit limits on the behavior of individuals. Authority holders are expected to act in a manner consistent with the predominant value system of the society. These social limitations are major factors in shaping the zone of acceptance and the general cultural deference of individuals who are members of organizations.
4. Physical limits. An authority holder can neither force a person to do something that is simply beyond that person’s physical capabilities nor escape the natural limits of the physical environment, such as climate or physical laws.
5. Technological constraints. The advances and the limitations of the state of the art must be considered in the exercise of authority; no amount of power or authority can bring about a result that is beyond the technical ability of the individuals.
6. Economic constraints. The scarcity of needed resources limits the behavior of formal authority holders.
7. Zone of acceptance of organization members. Both authority and power have their limits in that the net cost of using either must be calculated. When a weak manager is faced with a strong employee group, perhaps as encountered in a strong union setting, the cost of using even legitimate authority may be too high; the authority grant is actually diminished.
Although many employees do not have complete freedom to choose what they will or will not do, they may resist authority in subtle ways, such as adherence to job duties exactly as stated in the job description, passive resistance, and failure to take initiative in any area not specifically designated by the supervisor. The manager must move into a distinct leadership position to develop a wide zone of acceptance, as leadership becomes an essential adjunct to the exercise of authority.
IMPORTANCE OF DELEGATION
Although the manager retains overall responsibility and authority for the work of the department or service, he or she must necessarily delegate authority to specific workers under his or her jurisdiction. Simply put, it is not possible for the manager to carry out every task. Therefore, each worker receives delegated authority from the manager to proceed on a day-to-day basis. Empowerment of the workers is essential.
Managers set up the parameters for action through several means: the development of policies and procedures, the promulgation of work rules and codes of behavior, the development of job descriptions with job duties and expectations well delineated, and the presentations of formal orientation and training programs associated with job duties. The manager consciously selects an appropriate style of leadership and communication to further enhance an atmosphere in which workers accept responsibility for their part in meeting the organizational goals.
A manager who is new to the role may experience some uneasiness with delegating. First, there is simply that natural tendency to think, “I can do this better or faster myself.” Second, a manager may harbor some fears. For instance, if the worker fails at the task, the responsibility still rests with the manager; it is the manager who will take the heat, so to speak. There is also a certain loss of satisfaction and recognition; managers are often removed from day-to-day interaction with patients and their families and their own professional peers who remain in the arena of active, hands-on practice. Recognition of these inner barriers to delegation is the first step to overcoming resistance to this necessary aspect of authority.
“Dos” and “Don’ts” of Delegation
Know when to delegate. In most day-to-day circumstances, delegation of authority is the norm. Routine tasks such as employee scheduling, for example, are easily accomplished by the supervisor closest to the unit. Certain highly specialized tasks such as revenue-cycle/compliance reviews are best delegated to a member of the department team who specializes in the area. Such a person would have the most up-to-date knowledge related to the topic. Workflow coordination and routine problem solving between or among working units are best accomplished by the immediate unit supervisors who are in continual interaction. Delegation is also a part of team development; the manager builds capability and confidence in the assistant managers, unit supervisors, and specialists. Delegation is part of the intentional training and mentoring goals of the manager.
Know when not to delegate. Certain activities remain the primary responsibility of the manager and normally are not delegated, such as hiring, disciplinary action, and termination. Generally, any task that falls under the heading of personnel management cannot be delegated; no nonmanagement employee must ever be empowered to make personnel decisions that affect other nonmanagement employees. Throughout each process, there will be input from unit managers and supervisors, but the final action is that of the manager. Complex or volatile employee or client situations sometimes arise; these, too, are the manager’s responsibility. Overall systems and workflow, along with equipment and layout, are the manager’s concerns, although there is input from unit managers and supervisors.
Avoid common pitfalls associated with delegation. Two common pitfalls can occur inadvertently; the prudent manager takes care to avoid these. First, a manager might undermine a unit supervisor by countermanding, even informally, a decision made by the first-line supervisor. For example, a unit supervisor might deny a request for a schedule change by an employee because of workflow or staffing considerations. The employee might informally ask the manager to approve the desired schedule change. Managers who allow themselves to override a subordinate manager’s decisions undercut the authority and responsibility grant of this manager. (This is not the same thing as the normal grievance or appeal process during which an employee may meet with a higher-level manager at designated steps in the course of the seeking resolution.) Second, a manager, with the best of intentions, solicits information on a regular basis, perhaps daily, from unit managers. The casual but purposeful question, “How are things going in your unit today?” may lead to on-the-spot reports of one or another workflow or staffing problem. The concerned manager might readily respond, “I’ll look into that and get back to you,” instead of involving the subordinate supervisor in solving the problem.
Interact with workers regularly. It is necessary to set up a balanced system of availability and support. The manager remains available to unit supervisors through a mix of formal and informal interactions, such as the following:
• Formal, periodic meetings with individual supervisors for in-depth feedback about a specific activity. These meetings focus on workflow and related problem solving.
• Formal development meetings with individual supervisors or the team of supervisors. The focus is development of supervisory skills, mentoring, and career path development.
• Informal day-to-day “prn” interaction.
• A combination of formal and informal daily briefing, sometimes referred to as “the huddle.”
The final practice involves a brief daily meeting, about 15 minutes in length, held sometime between the early morning and midday. By this time, any immediate concerns will have surfaced, yet there is sufficient time remaining in the day to solve most problems that arise. The team usually remains standing while each supervisor summarizes the particular concerns in his or her functional unit, allowing each member of the team to become aware of workflow impact, employee issues, and “news of the day.” Team members are able to make immediate plans to deal with intradepartmental concerns without the manager’s having to mediate such coordination. An administrative assistant also attends, bringing materials for distribution on the spot, which eliminates the accumulation of materials in the inbox for each team member. The manager comments on such materials if follow-up is required. The assistant’s presence also facilitates actions that keep things moving without further instruction—for example, he or she will follow up on a purchase order or check on a question relating to a payroll matter.
The manager typically rotates the location of “the huddle” among the different units of the department unless confidential information is involved. In the latter case, the unit supervisor of that department leads a roundtable briefing. This action provides visibility of the authority–responsibility mandate entrusted to that supervisor. The employees of the unit see their unit supervisor as a member of the team. Furthermore, this experience of leading a roundtable briefing provides additional training in leadership for each team member. “The huddle” takes place daily, even when the manager is unable to attend, thereby reinforcing the role set of the supervisors as designated agents of the manager. This practice empowers the unit supervisors by enabling them to take the lead.
Effects of Good Delegation
Recognition of the benefits of proper delegation and, conversely, awareness of the consequences of poor delegation further enhance a manager’s ability to delegate. Just as proper delegation increases the zone of acceptance on the part of employees, so failure to delegate demoralizes workers, thereby shrinking their field of cooperation. Morale suffers, turnover rates increase, and loss of productivity results. When workers in regular contact with clients cannot easily take immediate and effective action, client groups become alienated and unhappy and seek services elsewhere. The organization develops a reputation for being wrapped in bureaucratic red tape.
Finally, without proper delegation, a manager must remain constantly present to authorize action; this is time consuming and wasteful of managerial resources. It is also unrealistic because a manager’s duties frequently require being out of the department or office and even away from the premises. With a manager’s commitment to delegation in place, and with, the day-to-day activities flow toward accomplishing the overall mission of the organization.
LEADERSHIP
Frequently, when professionals describe a leader as a powerful person who has made it to the top of his or her field, they use the expression “industry leader” or other similar label. The successful health professional does not seem to share familiar and common habits with the average practitioner. People imagine the person as a romantic figure who is not human. Drucker describes leadership in reality as “mundane, unromantic and boring. Its essence is performance.”11 Yet leadership is vital for the future growth and development of health professions. This section is designed to address the leadership qualities that everyone has buried within. Rather than define leadership as distant and unusual, this section describes it as a set of characteristics that emerge from individuals who are able to get things done within an organization.
“Natural leaders” do exist, but it is likely that they are few and far between. For the most part leaders are not born; they develop. In fact, leaders are not extraordinary in any way except that they can match organizational goals to the abilities and interests of their work groups. This talent is mercurial; some leaders are effective in one set of circumstances but not in others. Leadership is not based on impossible characteristics possessed by few; rather, it is a collection of abilities that successful managers have carefully cultivated.
Definition of Leadership
A leader is a person who can organize tasks and make things happen through the efforts of a group of people. Using the unique interests and needs of every member of the work group, the effective leader inspires goal-directed behavior that is consistent and efficient. The leader cajoles, rewards, punishes, organizes, stimulates, strengthens, communicates, and motivates. There is no set standard for leadership behavior, as individuals must match their own characteristics to the needs of the organization.
The personal characteristics common to many leaders are a strong self-image, a vision of the future, a firm belief in the goals of the organization, the ability to influence the behavior of subordinates, and the ability to relate to and influence individuals in parallel or superior positions of authority.
Leadership exists both informally and formally. Informal leadership is exerted in many settings, including formal organizations. Within any formal organization, there are subunits and even para-organizations, such as collective bargaining units, that are led by individuals who do not hold formal hierarchical office. Leadership is implied, even explicitly included, in the role of the manager whose function is to achieve organizational objectives by coordinating, motivating, and directing the work group. For the remainder of this discussion on formal leadership, it is presumed that the manager is a leader in addition to being a holder of formal authority.
Where Do “Leaders” Come From?
The word “leaders” in this subheading stands in quotes because not all persons in leadership positions are truly leaders.
In organizational life, leaders are “acquired” in two ways: they are promoted from the ranks of employees, and they are recruited from outside of the organization. Both means have their advantages and disadvantages. The leader promoted from within ordinarily knows the organization and its structure and workings, understands the policies and practices of the organization, knows about the processes he or she will oversee, and is familiar with the staff. But the leader promoted from within usually has drawbacks to overcome in the form of interpersonal relationships that can hamper the transition into a leadership role, especially, as frequently occurs, when one is promoted to managing a department in which he or she was one of the employees.
The leader recruited from outside usually comes in with no knowledge of the personalities already in place. Depending on conditions existing before the new leader’s arrival, this person may be cautiously welcomed by the staff as one who can improve certain conditions or may be regarded with apprehension as a potential “new broom” who will make changes. So whether a new “leader”—whether first-line manager, middle manager, or whatever—rises from within or comes from outside, there are pluses and minuses associated with the appointment.
Anyone who has been part of a work organization for any length of time has learned that the best rank-and-file employees, those who are most knowledgeable and successful, do not necessarily make the best leaders. Yet there is a certain amount of logic in the promotion of the technically best employees into management. After all, promoting weak or even mediocre workers into management is surely not a consideration. But many leadership positions are filled by individuals who have had little or no education in the management of people. This is a large area of concern in many organizations, and it is often addressed through management development programs.
But rather than further consideration of where leaders come from, it is important to consider a related question that says a great deal about many individuals who enter leadership. Why do many individuals seek leadership positions?
What Drives People to Become Leaders?
There is an informal exercise that is worth conducting with a group of employees, especially with people in a supervisory development program who wish to become supervisors or have already been promoted to supervision. Lead them in a brainstorming exercise using this instruction; list any or all reasons a given individual might have for seeking a leadership position. Do not let the participants note just a few of the supposedly standard reasons, and do not be concerned with similarities and overlaps among reasons. Without too much prodding, a group of 10 or more people can come up with literally dozens of reasons why individuals seek leadership positions. Then have the group sort these reasons into two broad categories: (1) those addressing the true needs of leadership and (2) those addressing primarily an individual’s needs or desires.
It does not take too long to discover that the reasons addressing an individual’s needs or desires far outweigh the reasons that address the needs of the organization or entity that requires leadership. On the “up” side will be to make a difference, to serve the customer, to implement my ideas, to improve the organization, to motivate and encourage employees, to solve some long-standing problems, and a number of other similarly noble statements. On the “down” side, always the much longer list coming from this exercise, will be to make more money, to obtain better benefits, to acquire standing as a manager, to acquire power, to exert influence, to position myself to grow further, and other essentially selfish reasons. If asked, of course, one who is seeking a leadership position will never articulate any of the selfish reasons but will surely state a couple of the organization-positive reasons.
Consider the public arena in which we obtain leaders by voting for them. Candidates will tell us what they stand for and what they propose to do if elected (or, in these times of rampant negative campaigning, will regale us with reasons why their opponents are unfit to hold office). A candidate for public office will always articulate some variation on I only want to serve. But consider this question: would this individual still “want to serve” if doing so did not entail acquiring money, benefits, position, power, prestige, influence, acclaim, and such?
Thus, people seek leadership positions for both positive and negative reasons, and many of these reasons are driven by selfishness. It is possible that many of the best potential leaders are buried in the general population; these are people who have or could develop the requisite skills but experience none of the selfish urges or who simply do not want the responsibility of what they may see as a thankless job. Once in a while, in the face of an emergent situation when others have failed or become incapacitated, one of these potential leaders will step into the breach and take charge, but this does not often happen. However, seldom do these best potential leaders step forward and seek leadership positions.
Leadership Qualities
To influence and induce others to strive toward a goal, the leader must possess not only a strong vision of that goal but also the ability to render the goal meaningful to the group. The knowledge, insight, and skill of the leader are greater than those of other members of the group. At an obvious level, the leader leads but does not drag, coerce, or push the group. Group members are steadily induced to move toward the goal; they are influenced in a pervasive way so that the overall goal becomes their own goal. The leader does not achieve the work alone but instead successfully coordinates the work of the group. The leader inspires confidence through both emotional and knowledge ties with the followers. Indeed, a major factor that characterizes a truly successful leader is the willing acceptance of that leadership by the followers.
It is possible to generate a fairly lengthy list of qualities and characteristics that some would say “define” a leader. However, there are a couple of problems related to the creation of such a list. One difficulty, surely minor in the long run, is that no one person’s list is ever complete in the eyes of another person, and it approaches the impossible to get even a few people to agree on which qualities and characteristics are more important than the others. But the greater difficulty with any list of “essential qualities and characteristics of a leader” is that no matter what quality or characteristic is cited as “essential,” we can nevertheless point to some supposedly very successful “leaders” who are lacking in such. Many successful leaders are lacking, for example, in honesty, compassion, analytical ability, and numerous other qualities. So any attempt to define a leader by listing qualities and characteristics simply takes us back to the single characteristic that always holds true: the acceptance of the followers. One who is not accorded the acceptance of the followers does not truly lead but rather pushes.
Leadership Functions
In formal organizations, the leader has certain functions that are tied to the organizational need for leadership. The leader is expected to influence, persuade, and in general control the group. As an individual with vision, the leader is expected to take calculated risks and to act as a catalyst in the change process.
The leader carries out important functions on behalf of group members through the role of representative. For example, employees look to their unit or department head to speak for them and to seek or to obtain advantages for them. The leader may be cast in several roles by followers, especially at the symbolic level, and may even be seen as the father or mother figure who shields the individual from difficulties. The leader may also be the scapegoat. As the management representative closest to the rank-and-file worker, the first-line leader–manager bears the brunt of anger when the organizational situation is less than optimal.
The leader is presumed to embody the values of the group. As such, the leader becomes the focal point in the motivational process. He or she fosters the development of the climate and conditions that favor individual involvement in group effort. Leadership is a process more than a structure; the leader fosters the climate for change so that the organization will possess the adaptability required for long-term survival.
From Theory to Practice: A Leader’s Plan of Action
The manager must make a conscious commitment to the exercise of leadership through specific actions. Leadership activity clusters in natural groupings and to a considerable extent are intertwined. Here are some examples of leadership action relating to health information management:
1. The leader starts and sustains the conversation. By being out in front of the trends, the leader studies the big challenges, “digests them,” “talks them up,” and translates them into action plans within the organization. Examples include encouraging employee development through the attainment of additional specialty credentials and promoting participation in regional health information exchange and e-health initiatives.
2. The leader uses professional and technical competence to promote the health information professionals as the authoritative sources for clinical documentation systems and practices. Activities would typically include monitoring the federal initiatives concerning the electronic health record (EHR) initiative, the dissemination of information about the current changes in electronic discovery civil rule and the related topic of the definition of the electronic legal record, and serving as EHR project manager or team member.
3. The leader partners with key players in the organization. The leader identifies individuals whose support is critical to successful implementation of major systems—for example, the EHR, speech recognition technology, or computerized provider order entry. The leader takes the initiative in interdepartmental collaborative action such as:
○ Policy and procedure affecting joint action
○ Clinical pertinence review protocols
○ In-service training needs
○ Compliance reviews and billing audits
○ Risk management reviews
○ Interorganization peer review
4. The leader is actively engaged in the life of the organization. The leader recognizes and accepts that necessary work extends beyond the routine 9-to-5 day and beyond the borders of the department. The leader’s attitude is one of loyalty to and enthusiasm for the work of the organization. This visible support of the mission might take on a variety of forms:
○ Participation in organizational events to honor employees or volunteers—for example, employee recognition ceremonies and receptions
○ Participation in outreach activities such as career days, health fairs, and fund-raising events
○ Attendance at events sponsored by other departments—for example, the open house celebrating a designated professional week (such as Physical Therapy Week or National Nurses Week)
○ Participation in the organization’s speakers bureau
○ Hosting regional meetings of one’s profession to bring attention to the organization’s areas of excellence
5. The leader passes on the praise and the pride. Employees are not taken for granted; rather, their accomplishments are noted within the department and the organization. The leader takes care to nominate employees for appropriate awards such as “Employee of the Month.” Departmental activities are included in the internal newsletter, with its customary “spotlight on” column. The leader submits entries for trade and professional association newsletters featuring the department. The leader finds opportunities for employees to participate in extradepartmental events, such as annual disaster or emergency preparedness drills, thereby raising the visibility and involvement of the group.
Styles of Leadership
The manner in which a manager interacts with subordinates reflects a collection of characteristics that constitute a style of leadership. Although any manager may use several styles of leadership—choosing the style most appropriate for a given situation—one style generally emerges as that manager’s predominant mode of interaction.
Autocratic Leadership
Also referred to as authoritarian, boss-centered, or dictatorial leadership, autocratic leadership is characterized by close supervision. The manager who uses this style gives direct, clear, and precise directions to employees, telling them what is to be done and how it will be done; there is no room for employee initiative. Employees do not participate in the decision-making process. There is a high degree of centralization and a narrow span of management. The chain of command is clearly and fully understood by all. Autocratic managers use their authority as the principal, or only, method of getting work done because they believe that employees could not properly or efficiently carry out work assignments without detailed instruction.
There are two general types of autocratic leadership, exploitative and benevolent. In the exploitative type, the followers are literally exploited for the benefit of the leader. In the benevolent type, the “father-knows-best” approach to leadership is used; the leader treats followers kindly while sincerely believing he or she must make all the decisions and call all the shots. Both the exploitative autocrat, fortunately a seldom-encountered sort of leader, and the benevolent autocrat, a much more common sort than the other, are dictators; they lay down the law and the followers have no choice other than to comply or leave.
Although autocratic leadership appears to get results much of the time, it can be fatal in the long run. Employees can lose interest in their assignments and stop thinking for themselves, because there is no room for independent thought. Under certain conditions and with specific employees, however, a degree of close supervision may be necessary. Some employees prefer to receive clear and precise orders, because close supervision reassures them they are doing a good job. Even so, it can generally be assumed that an autocratic, close leadership style is the least effective and least desirable method for motivating employees to perform. This remains so whether the leader is the harsh exploitative autocrat or the kindly benevolent autocrat; in either case, the leader dictates and the followers are expected to comply.
Bureaucratic Leadership
Like the autocratic leader, the bureaucratic leader tells employees what to do and how to do it. The basis for this leadership style is almost exclusively the organization’s rules and regulations. For the bureaucrat, the rules are the law. The bureaucratic manager is often afraid to take chances and manages “by the book.” Rules are strictly enforced, and no departures or exceptions are permitted. The bureaucrat, like the autocrat, allows employees little or no freedom. Some bureaucrats become so entrenched in their reliance on rules and regulations that they are essentially paralyzed when encountering a situation for which there is no applicable rule or regulation.
Participative Leadership
In participative leadership, the contribution of the group to the organizational effort is emphasized. This style is the opposite of autocratic, close supervision. The manager who uses the participative method involves the employees in the decision-making process and in the maintenance of cohesive group interaction. The manager involves employees in determining goals, objectives, and work assignments, and similarly he or she involves them in defining the nature and extent of a problem before making a final decision and issuing directives or orders. This approach endeavors to make full use of the talents and abilities of the group members. If approached honestly and with fair consideration of employees’ input, the employees who have participated in the process are likely to experience a sense of ownership in the resulting decision.
Participative management does not weaken a manager’s formal authority, because the manager remains responsible for the final decision whether it is made independently or by the group. The obvious advantage of the participative style of leadership revolves around the meaningful involvement of the employees, which greatly enhances the implementation of the decisions that have been made.
Consultative Leadership
Some managers use a pseudo-participative method of leadership to give employees the feeling that they have participated in decision making. The consultative leader routinely solicits employee input, then just as routinely ignores that input and independently makes the decision. This sort of leader is often self-deluded into believing that he or she is being openly participative by soliciting employee input. However, when the employee input is ignored, employees quickly sense that the manager is manipulating people and that their participation in the decision-making process is not real.
Laissez-Faire Leadership
Laissez-faire or “free rein” or essentially “hands-off” leadership is based on the assumption that individuals are self-motivated and generally self-directed. In this approach, employees receive little or no supervision. Employees, as individuals or as a group, determine their own goals and make their own decisions. The manager, whose contribution is minimal, acts primarily as a consultant and does so only when asked. The manager does not lead but allows the employees to lead themselves. Some managers consider this approach to be true democratic leadership, but the usual end result is disorganization and chaos. The lack of leadership permits different employees to proceed in different directions.
Paternalistic Leadership
This is quite similar to benevolent autocracy, the “father-knows-best” approach to leadership. The paternalistic manager treats employees like children, telling them in a kindly manner what to do and how to do it. It is the paternalistic manager’s belief that employees do not really know what is good for them or how to make decisions for themselves. In this approach, everyone is watched over by the benevolent manager—the benign dictator—and the employees eventually become extremely dependent on their “paternalistic boss.” The paternalistic leader genuinely believes that the followers are incapable and must therefore be told every move to make. In contrast, the benevolent autocrat does not care whether the followers are capable or not, but firmly believes that he or she must think and decide for the entire group.
Continuum of Leadership Styles
Another way to view leadership behavior is on a continuum ranging from highly boss-centered to highly group-centered. The relationship between the manager and the employee in the continuum ranges from completely autocratic, in which there is no employee participation in the decision-making process, to completely democratic, in which the employee participates in all phases of the decision-making process. The following briefly describes the gradations along the continuum:
1. The manager makes the decision and announces it. The manager identifies a problem, considers alternative solutions, selects a course of action, and tells employees what to do. Employees do not participate in the decision-making process; they do not provide input in any form.
2. The manager “sells” the decision. The manager again makes the decision without consulting the employees. Instead of simply dictating the decision, however, the manager attempts to persuade the employees to accept it largely through explaining how the decision serves both the goals of the department and the interests of group members.
3. The manager presents ideas and invites questions. The manager has already made the decision but asks the employees to express their ideas. Thus, the manager allows for the possibility that the initial decision may be modified.
4. The manager presents a tentative decision subject to change. The manager allows the employees the opportunity to exert some influence before the decision is finalized. The manager meets with the employees and presents the problem and a tentative decision. Before the decision is finalized, the manager obtains the reactions of employees who will be affected by it.
5. The manager presents the problem, obtains suggestions, and makes the decision. Up to this point on the continuum, the manager has always come before the employees with at least a tentative solution to the problem. At this point, however, the employees get the first opportunity to suggest solutions. Consultation with the employees increases the number of possible solutions to the problem. The manager then selects the solution that he or she regards as most appropriate in solving the problem.
6. The manager defines limits and asks the group to make the decision. For the first time, the employees make the decision. The manager now becomes a member of the group. Before doing so, however, the manager defines the problem and the limits and boundaries within which the decision must be made.
7. The manager permits subordinates to function within the limits defined by the superior. For the maximum degree of employee participation, the manager defines the problem and lists the guidelines and boundaries within which a solution must be achieved. The limitations imposed on the employees come directly from the manager, who participates as a group member in the decision-making process and is committed in advance to implementing whatever decision the employees make.
In summary, the manager’s relationship with the employees influences morale, job satisfaction, and work output. Employee satisfaction is positively associated with the degree to which employees are permitted to participate in the decision-making process. In contrast, poor supervision causes employee dissatisfaction, high turnover rates, and low morale.
Factors That Influence Leadership Style
No one style of leadership fits all situations. A successful manager is one who has learned how to apply the most appropriate method for a given situation. Before selecting a style of leadership or deciding to blend several styles, the manager must consider a number of factors:
1. Work assignment. If the work assignment is repetitious, properly trained employees do not need constant or close supervision. If the assignment is new or complex, however, close supervision may be required.
2. Personality and ability of employees. Employees who are not self-starters function best under close supervision. Others, by reason of personality and work background, can take on new and important responsibilities on their own; these individuals react best to participative leadership. The occupational makeup of a department may also influence the leadership style used by the manager. For professional practitioners (e.g., physical therapists, occupational therapists, health information personnel) or other highly skilled employees, the employee-centered participative leadership style is often most effective. When employees are unskilled or unable to act independently, the boss-centered or autocratic style of leadership may produce better results.
3. Attitude of employees toward the manager. The manager cannot begin to lead or influence behavior unless he or she is accepted by the group. Employees fully accept the manager’s authority only when they believe that the goals and objectives of the manager are consistent with their own personal and professional interests.
4. Personality and ability of the manager. The manager’s personality has a definite effect on the behavior and performance of employees. The manager must treat employees’ opinions and suggestions with respect and must sincerely encourage employee participation.
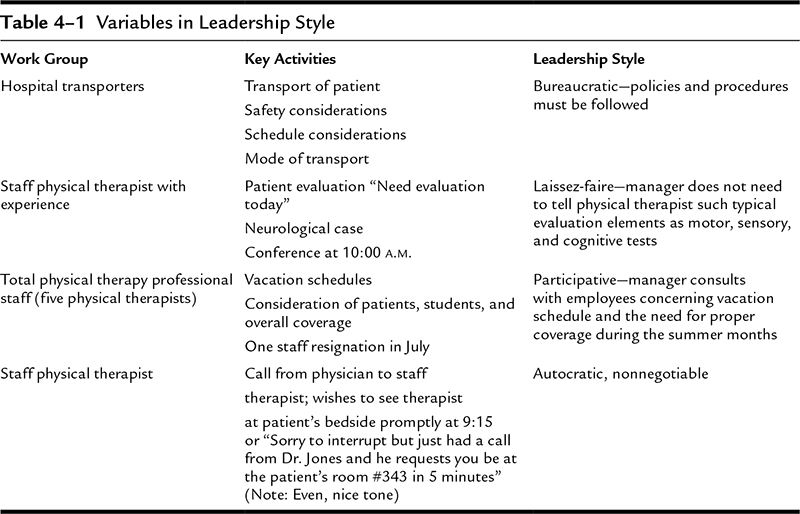
When faced with different work group encounters and situational factors, the effective manager shifts from one style of leadership to another, often without conscious recognition of a shift in style. Table 4–1 shows examples of the adjustments in leadership style that a manager makes to stimulate maximum effort from employees.
Communicating Your Own Managerial Style
A manager may deliberately go out of his or her way to communicate to employees the style of leadership or management he or she practices. It is not particularly uncommon for a manager who is relatively new to an organization or department to make statements such as these: “I believe in employee participation, and I always welcome your input”; “I practice management by wandering around, so you’ll see me a lot in the departments”; or, one of the most oft-heard, “my door is always open.”
There are some significant hazards in introducing yourself as a manager in such a manner. In the words of a wise, anonymous observer of management practices, “It’s Management 101—using the buzzwords, saying what you think you should be saying, telling people that you’re what the ‘management experts’ say you should be.” The hazards inherent in such pronouncements are found in the risk of being trapped by employee perception.
It takes only a few perceived contradictions of your self-described style to create dissonance. As soon as you are seen unilaterally making decisions without soliciting participation or input, you have created a perceived conflict between your words and your actions. And when a few employees have found you unavailable, although you have said “My door is always open,” more such conflicts are created and employee perceptions begin to turn unfavorably against you, whether deservedly or not. Any given perception may not be entirely accurate, but to the perceiver perception is reality.
It is best to say as little as necessary about your own style of leadership and allow your actions to convey your true style. In other words, instead of telling employees what kind of leader you are, let your actions show them. You may not come across as the sort of leader idealized in “Management 101,” but, even more importantly, you are more likely to come across as honest.
Situational Leadership and Adjustment
What is here referred to as “situational leadership” is hardly worth of a label in its own right. For the well-experienced conscientious manager and insightful leader of people, it should be automatic. Situational leadership consists of adapting one’s style to the particular situation at hand or to the unique needs of the moment.
Not every problem submits to the same logical process of analysis and solution. Not every need that arises in the workday can be addressed in an identical manner. And, most important to the manager, not every employee is able to respond as desired to the same management approach. Within the same group you may have “Theory X” individuals, who must be led and who indeed often prefer to be led and have others do their thinking for them, along with “Theory Y” people who are self-motivated and capable of significant self-direction. This is especially likely in department employing both professionals and nonprofessionals. Although the same overall “rules”—that is, the same personnel policies—apply uniformly to all employees, the manager will have to deal differently with individuals in other ways. Some you may consult and invite their participation or input; others you will simply direct.
Avoid making assumptions about people; never assume that what works with one will work with all others. Know your employees and try to understand each one as both a producer and a person. By working with people over a period of time, and especially by working at the business of getting to know them, you can learn a great deal about individual likes and dislikes and capabilities. Learn about your people as individuals and when necessary lead accordingly. If you are convinced that a certain employee genuinely prefers orders and instructions and this attitude is not inconsistent with job requirements, then use orders and instructions. Although many employees of healthcare organizations seem to prefer participative leadership, not everyone will desire this same consideration. Maintain sufficient flexibility to accommodate the employee who wants or requires authoritarian supervision. It is fully as unfair to expect people to become what they do not want to be as it is to allow a rigid structure to stifle those other employees who feel they have something more to contribute.
There is no single style of leadership that is appropriate to all people and situations at all times. Let the situation and the needs of those involved dictate your managerial style.
SOME FINAL THOUGHTS ABOUT AUTHENTIC PERSONAL LEADERSHIP
In the preceding discussion, the manager has been identified as an agent of change. The functions of the manager have been noted, and leadership traits and foundations have been explored. All of this leads up to some final thoughts about the manager–leader as a person.
One who would aspire to leadership and become successful in its pursuit must perform some serious self-examination by asking: why should anyone be led by me? This can be a startling question. A person’s initial reaction might be one of defensiveness or even irritation: “Shouldn’t it be obvious? I am up-to-date in my field; I come in every year at or under budget; no accreditation citations arise from my department; there are few, if any, grievances from my staff; and my employee turnover is minimal. What more do they want?”
Now ask the latter question another way: “What more do you want? What kind of person are you striving to be?” Some people view the idea of self-development as trendy: dress for success, or six steps to persuading and negotiating, or similar topics suggesting artificial methods for getting ahead in the organization. Such practices even become the fodder for sit-coms and cartoons, not to be taken seriously. But for others, this focus on self is embarrassing and perhaps discouraging. Who can be the perfect person?
Such reactions could cause us to neglect this important aspect of leadership. Notice the emphasis that major business and management schools place on the cultural, spiritual, and psychological development of the manager–leader. They devote significant curriculum time and resources to these topics. Major business and management journals include regular features on these aspects of leadership. When we observe successful peers, higher-level managers, and leaders both within the organization and external to it, we notice some common traits. Specifically, they possess a set of value-added characteristics.
Value-Added Characteristics
The value-added characteristics flow from a deep respect for the dignity of the human person. This genuinely high regard for oneself and for others is reflected in the presentation of self in everyday life. It is manifested through an attitude of engaged, conscious living; gracious interpersonal relationships; and calm, orderly work habits. It is embodied in the values of integrity, trustworthiness, and respect.
Engaged, Conscious Living
Individuals who display the characteristic of engaged, conscious living have an awareness of and an enthusiasm for life. They bring positive energy to the work setting that is rooted in a balanced life—they like their life! Their approach to life keeps them from overreacting. They are not the caricature characters who are always having a bad day and give off the negative vibration: “don’t even ask; you don’t want to know; wait until I have had my coffee.” No, these are the people who are steady; they are pleasant to associate with; they easily and routinely show graciousness.
Gracious Interpersonal Relationships
In an age of depersonalization, coupled with overly casual ways of relating, a person can inadvertently fail at fundamental politeness. The antidote is gracious interpersonal relationships. The gracious person truly sees you and acknowledges you; a simple “good morning” is extended to coworkers, and a cordial “hello” is given to the attendees at a meeting. This person knows how to make an introduction, both informal and formal, and can offer an appropriate blessing, a toast, or a congratulatory message at a celebratory occasion. He or she sends the timely handwritten note and does not fall into the casual practice of cute, humorous, or even sarcastic commercial cards. He or she can make conversation with ease and does not rely on the latest sports headline as the only topic.
Calm, Orderly Work Habits
The workplace is accepted for what it is—a place of business. The attentive manager–leader maintains an orderly work space, free of distracting items (e.g., mementos, knickknacks, highly personal possessions). The office is not the person’s second home. The work at hand is laid out for attention and then returned to its proper holding place. A member of the organization who comes to this person’s office can literally sit down without having to step over or move “files and piles.” If a high-level manager brings a visitor to the office space, it should not result in embarrassment on anyone’s part. There is an attitude of dignity and respect toward one’s physical environment; this person is a good steward of the material goods entrusted to him or her.
Embodiment of Values
Others can easily make positive remarks about these manager–leaders. They have integrity; they promote ethical behavior that is reflected in routine practice. There is no bootleg software in use. Their expense reports are truthful and straightforward. When given the opportunity to attend conferences and training sessions, they actively participate, take the opportunity to obtain information from vendors, and make useful contacts through networking. They are trustworthy; such a person can keep a confidence, and he or she is a thoughtful sounding board and a safe haven for letting off steam. The person confiding in this manager–leader knows that the conversation will be safeguarded.
Finally, these manager–leaders are respectful of others. People know that they are psychologically safe in such a person’s presence. People know they will not be recorded, photographed, or “uploaded” onto the various social media. The respectful manager–leader truly listens to the individual in one-on-one situations and at meetings; he or she is not doodling, knitting, clock watching, surreptitiously checking for messages, or multitasking. Attentiveness, being fully present, is the hallmark behavior of such a person.
Recall the probing question: Why should anyone be led by you? The answer becomes easy and obvious when one attends to purposeful self-development.
CASE: AUTHORITY AND LEADERSHIP: RISING FROM THE RANKS
Background
After working 8 years as a staff nurse on a general medical–surgical unit, Julie Davis was appointed nurse manager of that unit. Following a staff meeting at which her promotion was announced, Julie found herself surrounded by three longtime coworkers offering their congratulations and making other observations and comments.
“I’m really happy for you,” said Sarah Johnson. “This sounds like a terrific career step. But I suppose this means our carpool is affected, since your hours are bound to be a lot less predictable from now on.”
Elaine Rowe said, “And I guess that shoots the lunch bunch, too. Management commitments, you know.” The emphasis on management was subtle though undeniable, and Julie was not at all sure that she was pleased with what she was hearing.
Jane Davidson offered, “Well, maybe now we can get some action on a few age-old problems. Remember, Julie, you used to gripe about these things as much as the rest of us.”
“We’ve all complained a lot,” Sarah agreed. “That’s been sort of a way of life around here.” The tone of her voice shaded toward a suggestion of coolness and her customary smile was absent when she added, “Now Julie’s going to be in a position where she can do something, so let’s hope she doesn’t forget who her friends are.”
Elaine and Jane looked quickly from Sarah to Julie. For an awkward 10 seconds or so, no one spoke. At last, someone passing by said something to Julie, and as Julie turned to respond, Elaine, Jane, and Sarah went their separate ways.
Instructions
1. Identify the potential advantages Julie might enjoy in becoming manager of a group of which she has long been a member, and contrast these with the possible disadvantages that might present themselves because she has long been a member of this group.
2. Describe how you believe Julie will have to proceed in establishing herself as the legitimate possessor of supervisory authority on the unit, and describe the sources and forms of Julie’s authority.
CASE: DISCIPLINE AND DOCUMENTATION—HERE SHE GOES AGAIN
Background
“I’ve come to the end of my patience with Roberta Weston,” said accounting manager Sam Best. “The position she’s in is so important to us that we simply can’t afford any more of her omissions or mistakes. For the sake of the hospital and the department, I believe she’s got to go.”
“What’s the problem?” asked Charlene Harrison, the human resources director.
“Problems, plural,” Best answered. “She’s so late in posting receipts on rentals in the medical arts center that we wind up double-billing a number of physicians every month. Actually, it’s the same with just about all miscellaneous income—since she’s responsible for all receipts except third-party reimbursement. We’re losing control of income, and I get three or four complaints a week from people who claim they’ve been billed again for charges they’ve already paid.”
Best shook his head and added, “I’ve really tried to give her every chance to turn around, but nothing seems to work. At least not for very long.”
Harrison said, “I’ve reviewed Roberta’s file. The only evidence of a problem I found was your rather detailed performance improvement review of 2 months ago. In that process, you’re supposed to give the employee detailed direction aimed at correcting the problem. You did that, and you also provided a warning that task performance would be monitored closely for 30 days and that she could be let go by the end of that period if her work didn’t come up to satisfactory levels. You did the review well, but I didn’t see anything about any follow-up.”
Best said, “That’s because she had shaped up by the end of the 30 days.”
“But now she isn’t working up to the requirements of the job?”
“No. Her work was just marginally okay at the end of the 30 days, but within 2 weeks the bottom dropped out again and the mistakes started rolling in.”
Harrison asked, “What do you mean by ‘again’?”
“This is the third time I’ve been through this with her. I go over the areas in which she’s not working up to standard, she puts on a burst of effort and does better, and a month or so later she falls back into her old ways.” Best frowned and added, “I can’t put up with it any longer. Three strikes—she’s out.”
Harrison said, “According to her file, it’s just one strike. The only documentation is your single performance improvement review. What about the other two times?”
“Strictly verbal.”
“You didn’t write up anything? You’re supposed to cover such discussions with a counseling form or at least a memo for the record.”
Best said, “If I wrote up one of those every time I had to talk to an employee, I’d never get done writing. It’s a lot of work.”
“I know it is,” responded Harrison, “but you’ve got to have your documentation. As it stands right now, if we terminate her she could probably give us a real hard time with a couple of outside agencies.”
“So what should I do?” Best asked.
Instructions
1. Describe the ways in which the employee might be able to give the organization a “real hard time” if she is terminated now.
2. Develop a plan of action that you would recommend Sam Best to follow in dealing with employee Roberta Weston.
NOTES
1. Chester Barnard, The Functions of the Executive (Cambridge, MA: Harvard University Press, 1968), 167–169.
2. Herbert Simon, Administrative Behavior (New York, NY: Macmillan, 1965), 12.
3. Ibid., 129.
4. Robert Presthus, “Authority in Organizations,” in Concepts and Issues in Administrative Behavior, edited by Sidney Mailick and Edward H. Van Ness (Englewood Cliffs, NJ: Prentice-Hall, 1962), 122.
5. Edgar H. Schein, Organizational Psychology (Englewood Cliffs, NJ: Prentice-Hall, 1965), 11.
6. H. H. Gerth and C. Wright Mills, From Max Weber: Essays in Sociology (New York, NY: Oxford University Press, 1946), 196–204.
7. Ibid.
8. H. C. Metcalf and L. Urwick, eds., Dynamic Administration: The Collected Papers of Mary Parker Follett (New York, NY: Harper, 1942).
9. Ibid.
10. Ibid.
11. P. F. Drucker, “Leadership: More Doing Than Task,” Wall Street Journal (January 6, 1988).
CHAPTER 5
Planning and Decision Making
CHAPTER OBJECTIVES
• Define the management functions of planning and decision making.
• Identify the characteristics of plans and specifically address those characteristics or features that make plans effective.
• Identify participants and their responsibilities in the planning process.
• Delineate the constraints placed on planning and identify the boundaries to be observed in the planning process.
• Define and differentiate among the terms philosophy, goal, objective, functional objective, policy, procedure, method, and rule.
• Delineate aspects of project management and 500-day plans.
• Determine how to evaluate a decision’s importance.
• Describe some of the tools and techniques available to aid decision making.
Planning is the process of deciding in the present what to do to bring about a desired outcome in the future. We might further qualify this description by referring to planning as the process of tentatively deciding what to do because we have no assurance of exactly what the future will bring.
Planning involves determining appropriate goals and deciding on the means to achieve them, making assumptions, developing premises, and reviewing alternative courses of action. It is the what, who, when, and how of alternative courses of action and of possible future actions. In planning, the manager contemplates the state of affairs desired for the future in light of what is known or can be inferred about the future. Any time people are looking ahead considering what to do in the future—whether that future is years or only minutes away—they are planning.
In the planning process, the step involving the choice among alternatives is the decision-making phase.
CHARACTERISTICS OF PLANNING
Planning is the most fundamental management function and logically precedes all other functions. Unplanned action cannot be properly controlled because there is no basis on which to measure progress, and organizing becomes meaningless and ineffective because there is no specific goal around which to mobilize resources. Decisions may be made without planning, but they will lack effectiveness unless they are related to specific goals.
Planning goes beyond mere judgments, because judgments involve the assessment of a situation but do not stipulate actions to be taken. Planning concerns actions to be taken with reference to specific goals.
In planning, the ideal state is first identified. The initial approach to achieving that ideal is then modified, refined, and brought to a practical level through a variety of derived elements, such as intermediate target statements, functional objectives, and operational goals. Planning includes the decision-making process, particularly in the commitment phase. Logical planning includes commitment in terms of time and actions to be taken. There is a hierarchy in the process that includes the relationship of derived plans to the master course, the linkage of short-range and long-range plans, and the coordination of division and department or unit plans with those of the organization as a whole. Finally, planning is characterized by a cyclic process in which some or many goals and specific objectives are recycled.
In a sense, some plans are never achieved completely; they are continuous. For example, the goal of healthcare institutions to provide quality patient care is a continuing one that invests the many derived plans with a fundamental purpose. This goal is recycled during each planning period.
PARTICIPANTS IN PLANNING
Top management sets the basic tone for planning, determines overall goals for the organization, and provides direction on the content of policies and similar planning documents. This is not done in isolation but is based on information provided through the feedback cycle, through reports and special studies, and through the direct participation of personnel in each department or division. The manager consults the major superusers, both in the direct patient care divisions and the administrative units.
Department heads are normally responsible for the planning process in their areas of jurisdiction. They identify overall goals and policies for their departments, and they develop immediate objectives, taking into account their departments’ particular work constraints. In some organizations, a special planning department is created, such as a program and development division or a research and development unit.
Occasionally, clients participate in the planning process; such participation is required in some externally funded programs. In healthcare planning, for example, members of the provider, consumer, and business community are included at each level of the review process. Professional associations frequently involve their members in the planning process at local, regional, state, and national levels. Employee involvement is yet another aspect of participation. Organizations whose members belong to collective bargaining units involve employee representatives in formulating certain aspects of planning, such as plans to downsize or to change major patterns of staffing. Because the final responsibility for planning, with the attendant legal considerations, rests with management, the input of employees and the public is advisory in nature. Their roles should be well delineated at the outset, and their input is encouraged.
THE PLANNING PROCESS
Because planning is intended to focus attention on objectives and to reduce uncertainty, there must be a clear statement of goals. Once the goals to be attained have been established, premising must be developed—that is, the assumptions must be identified, stated, and used consistently. Premising includes an analysis of planning constraints and a statement of the anticipated environment within which the plans will unfold. In a healthcare organization, the premises reflect the level of care, the specific setting (e.g., outpatient clinic, inpatient unit, or home care), the specific number of beds per service, the anticipated number and kinds of specialty services or clinics, morbidity and mortality data for the outreach territory, and the availability of related services.
The department head states the premises on which departmental plans are based—for example, the number of inpatient beds, the readmission rate, the projected length of stay, and the interrelationship of the workflow. The following is an example of specific planning premises or assumptions based on the operation of a physical therapy service:
1. Anticipated hours of operation
a. 6 days per week
b. 8-hour day; evening coverage for selected patients and clinics
2. Anticipated caseload
a. Inpatients—100 per day
b. Outpatients—120 per day
3. Diagnostic categories
a. Hemiplegics
b. Arthritics
c. Amputees
d. Fractures
e. Sports injuries
4. Patient characteristics
a. Adults: general adult population; workers’ compensation/industrial health referrals; frail, elderly people; juveniles, especially those with sports-related injuries
b. Children
5. Level of care
a. Acute
b. Subacute
c. Convalescent
d. Chronic
Alternative approaches to reaching the desired state are developed, and the choices to be made are stated. Commitment to one of these choices constitutes the decision-making phase. Derivative plans then are formulated, and details of sequence and timing are identified. Planning includes periodic checking and review, which leads to the control process. Review and necessary revisions of plans, based on feedback, are the final steps in the cycle of planning.
PLANNING CONSTRAINTS OR BOUNDARIES
To constrain means to limit, to bind, to delineate freedom of action. Constraints in planning are factors that managers must take into account to make their plans feasible and realistic. Constraints, which are both internal and external, take a variety of forms. Analysis of the organizational environment by means of the clientele network, specifically the category of controller, leads to ready identification of planning constraints. The use of the input–output model also yields practical information about the constraints specific to an organization. The cost of data gathering and analysis is another constraint; if committees or special review groups are involved, the cost of their time must be considered.
General resistance to change impedes the planning process so that standing plans take on the force of habit. Without a program for regular review of plans, they become static and rooted in tradition. Precedent becomes the rule, and the bureaucratic processes become entrenched. The phase in the life cycle of the organization also affects planning, as the degree of innovation that is appropriate varies with each phase.
The nature of the organization also shapes the planning process. The extent to which the organization’s members participate in planning correlates with the predominant mode of authority. Highly normative organizations tend to include more member participation in their planning than do coercive ones. Ethics and values of the larger society, of the individual members, and, in health care, of the many professional organizations help shape the goal formulation and subsequent policies and practices. When health care is seen as a right and not as a privilege, there may be a greater openness to innovation and a demand for outreach programs and flexible patterns of delivery of service.
Within the organization, interdepartmental relationships may be constraints. In highly specialized organizations with many services or departments, each unit manager must consider how other departments’ needs and processes are interwoven with those of the manager’s own department. Effective planning includes an assessment of such factors. The manager sometimes must accept as inputs or constraints the procedures and policies of another department.
Capital investments must also be considered. When a major commitment that involves the physical layout of the facility or some major equipment purchase has been made, the degree of flexibility in changing the process is necessarily limited.
External factors to be considered in planning include the political climate, which varies in its openness to extensive programs in health care. The general state of labor relations and the degree to which unionization is allowed or perhaps even mandated in an industry may be imposed on the organization. The many regulations, laws, and directives constitute another set of constraints.
In healthcare organizations, the many legal and accrediting requirements are specific, pervasive constraints that affect every aspect of planning. Such requirements can be developed into a reference grid for the use of the manager, as compliance with these mandates is a binding element in the overall constraint on departmental functioning.
An alternative approach to the identification of constraints in any healthcare planning situation is the systematic recognition of the following major factors. (Also recall the earlier discussions on the settings and trends, and on response to change, for additional examples.)
1. General setting. The level and particular emphasis of care must be determined. For example, the goal of one institution may be acute care in specialized diagnostic categories; the goal of another may be long-term care of frail, elderly people. The critical organizational relationships that stem from the general setting should be identified (e.g., the institution’s degree of independence versus its adherence to corporate and affiliation agreements and contractual arrangements). Physical location may also be a constraining factor, although an earlier decision to develop the facility in a specific location may be part of the ideal plan. For example, the decision to develop a pattern of decentralized care so as to enhance the outreach program of a community behavioral health center will serve as a constraint on many derived plans, such as workflow and staffing patterns. Information about the general setting is readily available in long-range planning documents, licensure and accreditation surveys, annual reports, and public relations materials.
2. Legal and accrediting agency mandates. Each healthcare institution is regulated by a federal or state agency that imposes specific requirements for the level of care and nature of services offered. For example, a hospital is licensed by the state only after it meets certain requirements; it is approved for participation in the Medicare and Medicaid programs only after it fulfills certain conditions. In addition, a hospital must comply with special regulations for medical care evaluation. It also must comply, at a minimum, with malpractice insurance regulations and related risk management programs as well as fire, safety, and zoning codes.
3. Characteristics of the clients. The general patterns of mortality and morbidity for a given population must be considered, as well as related factors such as length of inpatient stay, frequency of outpatient services, emergency unit usage, and readmission rate. Patient sources of payment relate to the stability and predictability of cash flow. Specific eligibility for treatment may be another factor, as in certain services for veterans or programs for other specific groups. Demographic profiles for the area served and the organization’s internal database are the usual sources of such information.
4. Practitioners and employees. The licensure laws for healthcare practitioners and physicians, as well as the many federal and state laws pertaining to most classes of employees, govern the utilization of staff. These include the Labor Management Relations Act (Taft-Hartley Act), the Civil Rights Act, the Age Discrimination in Employment Act, the Unemployment Compensation and Workers’ Compensation Acts, the Occupational Safety and Health Act, and the Americans with Disabilities Act. The personnel practices mandated in the accrediting agency standards and guidelines of health agencies and professional associations also must be followed. Any contractual agreement resulting from the collective bargaining process must be taken into account. The specific bylaws and related rules and regulations for medical staff and allied healthcare practitioners are yet another constraint on plans involving employees and professional practitioners in any role.
Strategic or Limiting Factors as Constraints
Chester Barnard, in his classic work on the functions of managers, stressed the importance of identifying those limiting factors that constrain the development of plans.1 Legal and accreditation requirements and contractual agreements are major examples of binding constraints. The planning team identifies these factors to prevent a waste of time and energy in the planning process; they concentrate on developing plans that are feasible. Alternative solutions are narrowed to include only those that fit the organizational goals and the availability of resources, and that satisfy the binding requirements. In exceptional situations, managers might seek exemptions from the existing regulations so as to undertake a pilot program or demonstration project focusing on innovative practices, but this is rare.
CHARACTERISTICS OF EFFECTIVE PLANS
Effective plans are flexible. Plans should have a built-in capacity to change; they should be adaptable. A plan could include a timetable sequence, for example, that allows extra time for unexpected events before the plan goes off-schedule.
The manager seeks to balance plans so that they are neither too idealistic nor too practical or limited. On the one hand, plans that are too idealistic tend to produce frustration because they cannot be attained; they may become mere mottoes. On the other hand, plans that are too modest lack motivational value, and it may be difficult to muster support for them. Clarity and vagueness must also be balanced in formulating plans. These factors help make the goals realistic. A precise goal may be a motivational tool because it provides immediate satisfaction, but there is also merit in a degree of vagueness because with some plans, especially long-range ones, it may not be possible or desirable to state goals in precise terms. Vagueness can contribute to motivation by permitting the development of detailed plans by those more directly involved in the work. Finally, vagueness can provide the necessary latitude to compromise when this is required or is a general strategy in the development of plans throughout the organization.
Anticipating Changes and Updates in Existing Plans
The effective manager monitors the planning process as an ongoing activity so that existing plans may be modified and new plans developed to meet changes in one or several planning constraints. The manager is not caught unaware but instead has an active plan to monitor potential change. Federal and state agencies as well as accrediting agencies issue their intended changes well in advance of their required implementation. Some agencies issue annual or semiannual agendas of changes under consideration. The various inspectors general regularly make known the targeted review focus for the upcoming year.
Plans needing modification are similarly assessed. As a manager identifies a trend or issue, he or she checks existing objectives, policies, and procedures to adjust them accordingly. An equipment recycling program may have worked well in the past, but now more particular attention is required when computers are recycled or destroyed; privacy considerations as well as environmental protection requirements need to be added as factors in such a recycling or disposal process.
Planning for the Unknown
In addition to planning based on well-known planning premises (e.g., expected number of patients per year, usual length of stay), planning for unknown events must be accomplished. The management team typically assesses the relative unknowns and seeks to make them progressively tangible. Although complete certainty is not possible, plans for rare but probable events are not only prudent but often mandated by external agencies. The strike plan is one such example. As the contract period for a given labor union agreement concludes, it is possible that a new contract may not have been agreed to yet. The workers may strike, thereby causing work disruption. Because patient care is of primary importance, management must have a contingency plan in place well before the strike deadline. Weather-related disruptions are another instance of possible-to-probable events. Managers in hurricane-prone locations or in regions with winter storms of a crippling variety have plans in place to cover those circumstances. Although managers do not know precisely how many or when such disruptions will occur, they have anticipated them well in advance and only need to fine-tune the plan when the emergency conditions escalate.
Disaster preparedness is a prime example of planning for the unknown. The types of possible disasters (e.g., epidemic, mass casualty, bioterrorism) are identified and the plans rehearsed in great detail precisely because their incidences are so unpredictable. Continuity of operations and plans for succession are essential aspects of disaster planning. These plans include such topics as alternative care sites, triage, changes in staffing patterns, and remote work site/telecommuting arrangements.
Each critical function of patient care and administrative support (e.g., food, electricity, water, medications, supplies) is assessed to determine the quantities of inputs needed and the vendors and suppliers available to meet those needs. An authority–responsibility pattern is developed for each critical function so that a clear chain of command is established, including succession plans indicating who will take over the tasks should the usual job holder become unable to function. The job descriptions and the training programs for the succession team members reflects these succession considerations. Plans should also include family well-being considerations (e.g., child care, elder care) so that workers with disrupted schedules may work without distraction and concern.
Types of Plans
The planning process involves a variety of plans that develop logically from the highly abstract, as in a statement of philosophy or ideal goals, to the progressively concrete, as in operational goals and procedures. Management literature on planning consistently includes the concepts of goals and objectives as central to the planning process. The terms goal and objective are frequently used interchangeably, except in discussions of management by objectives (MBO). The MBO concept refers to specific, measurable, attainable plans for the unit, department, or organization. For the purposes of this discussion of plans, the concept of goals will be discussed in terms of overall purpose. The concept of objectives will be discussed in terms of more measurable attainable plans, including unit or departmental objectives and functional objectives. Exhibit 5–1 lists the sequence of planning documents from planning state through controlling by means of operational goals.
EXHIBIT 5–1 Relationship of Types of Plans
| I. | Underlying Purpose/Overall Mission/Philosophy/Goal |
| II. | Objectives |
| III. | Functional Objectives |
| IV. | Policies |
| V. | Procedures V.1 Methods V.2 Rules |
| VI. | Work Standards |
| VII. | Performance Standards |
| VIII. | Training Objectives |
| IX. | Management by Objectives |
| X. | Operational Goals |
CORE VALUES, PHILOSOPHY, HERITAGE STATEMENT, AND MISSION
Individuals who share a common vision and set of values come together to create a formal organization for purposes that are consistent with and derived from their common values. The statement of core values, philosophy, or mission provides an overall frame of reference for organizational practice; it is the basis of the overall goals, objectives, policies, and derived plans. (See Exhibit 5–2 for a sample of a mission, vision, and values statement of a nonprofit, community-based healthcare center.) Actual practice, as delineated in policies and procedures, should not violate the organization’s underlying philosophy. As new members and clients are attracted to the organization and as the organization grows from the gestational to the youthful stage of the life cycle, the statement of principles may be made more explicit. A statement of core values may take one of several forms, such as a creed, a pledge, or a statement of principle. A heritage statement sometimes forms a sort of preamble to the core values statement, providing a context for the values and principles. This provides a context for the values to the historical development and long traditions of the founding/sponsoring organization. Here is an example of wording in a heritage statement:
EXHIBIT 5–2 Mission, Vision, and Values of Community Hospital
Community Hospital and Health Center exists to serve the community by providing expert, affordable, and readily available evaluation and treatment of the health needs of the residents. Educational and research activities to meet community needs and improve the quality of life of the communities we serve are part of our commitment.
Vision
Our vision is to offer health services ranging from primary to specialty care, with coordination among all units, thus encouraging patient care across the continuum of care. We seek to offer cost-efficient, customized care at our facility and to coordinate care with facilities in adjacent geographic areas. We seek partnership with the business, educational, and research communities for the mutual benefit of all.
Values
Our organizations govern our actions by the following values:
• Service: excellence and compassion in all aspects of care
• Unity: team approach among the direct care providers and support staff
• Innovation: continuous learning and searching for best practices
• Adaptability: proactive toward change and supportive of others who initiate change
• Communication: openness to receive information and feedback in a nonjudgmental atmosphere
Project Caring exists because the citizens of this county recognize their responsibility to care for those in need. From 1914 to 1965, services were largely organized around the institutionalized care of the aged, orphaned, and destitute. Since 1965, the project has expanded its programs to include social and community-based services. It relies primarily on charitable funding and depends on volunteers to help the professional staff.
In addition to reflecting the values of the immediate, specific group that formed the organization, a statement of philosophy may reflect, implicitly or explicitly, the values of the larger society. To one degree or another, for example, society as a whole now accepts the burden of providing for those who need medical care. The concept of health care as a right, regardless of ability to pay, gradually emerged as an explicit value in the 1960s. Emphasis on the rights of consumers and patients emerged in a similar evolutionary pattern in the 1970s. Because free enterprise is a benchmark of the democratic way of life, a trend toward marketing and competition in health care became a feature of the 1980s and 1990s. The early 21st century is characterized by a combination of all of these considerations.
Department managers in a healthcare organization are guided by several philosophical premises. These may differ from, and even be in opposition to, the managers’ personal values. However, as members of the executive team, the managers are expected to accept these premises. One of the goals of providing orientation and motivation is to foster acceptance of the underlying purpose of the organization. Typical philosophical premises in health care include the following:
• The basic philosophy of the group that sponsors or controls the healthcare institution (e.g., federal or state government agency, religious or fraternal organization, business concern)
• The guidelines promulgated by national associations regarding patient rights, safety and privacy, and similar issues
• Guidelines of accrediting agencies, such as The Joint Commission, that emphasize continuity of care, patient rights, and other topics
• Guidelines, codes of ethics, and position statements of professional associations (e.g., American Physical Therapy Association, American Health Information Management Association [AHIMA], American Occupational Therapy Association)
• Values of society in general, such as concern for privacy, equal access, employee safety, and consumer/client participation in decision making
• Contemporary trends in the delivery of health care, such as the shift from inpatient acute care to outpatient care and community-based outreach centers; the establishment of independent practices by health professionals (e.g., physical therapists) who formerly provided care only under the direct supervision of physicians; and the emergence of technical levels in several health professions and the acceptance of the care given by technicians
Mission statements usually remain stable over the life of the organization because the fundamental purpose of the organization remains unchanged. Note that there is another concept of mission, usually associated with military or emergency operations: the mission is specific and limited, and when completed, a new mission is undertaken. The concept of mission in this discussion refers to the relatively unchanging, underlying mission of the healthcare facility.
Medical centers devoted to acute care as well as teaching carry out an ongoing mission consisting of three elements:
• Educating superior physicians
• Enhancing research and knowledge
• Improving health care in the community and region
A specialty assisted living facility defines itself through its mission statement: to provide an assisted living residence for individuals in the early to middle stages of Alzheimer’s disease and other related memory impairments, in an environment of warmth, caring, safety, with the comforts and routines of home.
The following are excerpts from statements of philosophy. One health information department has its philosophy stated in a preamble:
Given the basic right of patients to comprehensive, quality health care, health information management, as a service department, provides support and assistance within its jurisdiction to the staff and programs of this institution. A major function of this department is to facilitate continuity of patient care through the development and maintenance of the appropriate health information systems, which shall reflect all episodes of care given by the professional and technical staff in any of the components of this institution.
An educational institution adheres to the following statement of philosophy:
One of the critical elements in an effective approach to health care is the establishment of the spirit and practice of cooperative endeavor among practitioners. Recognizing this need, the Consortium for Interdisciplinary Health Studies seeks to foster the team approach to the delivery of health care.
The following is from the statement of philosophy of a physical therapy department:
The physical therapy department as a component of the healthcare system is committed to providing quality patient care and community services in the most responsive and cost-effective manner possible. In addition, the department will participate in research and investigative studies and provide educational programs for hospital personnel and affiliating students from the various medical and health professions.
The philosophy of an occupational therapy private practice group is stated in these terms:
The Occupational Therapy Consultants, Inc. believe that humans are open systems that both influence and are influenced by the environment. Therefore, individuals are motivated to pursue goal-directed activities that reflect their values, roles, and interest. We use activities and environmental adaptations to provide positive reinforcement and a sense of mastery to our clients. We make “doing” possible.
The mission of this private practice group is as follows:
Occupational Therapy Consultants, Inc. will seek referrals from medical and nonmedical sources and offer high-quality, cost-effective services to clients and their caregivers whose roles, habits, and interests are limited by pathological, congenital, or traumatic incidents. Services, direct and consultative, will be offered in schools, homes, industrial settings, and outpatient facilities.
The values of the organization are stated explicitly in mission and vision statements. They are embodied in subsequent management practices and documents. Policies and practices for risk management, infection control, and in-service training are additional examples of vision and values informing day-to-day practice. For example in a sample labor union contract, the shared values of fostering patient care and providing good working conditions are amplified.
OVERALL GOALS
The goals of the organization originate in the common vision and sense of mission embodied in the statement of purpose or the underlying philosophy. They reflect the general purpose of the organization and provide the basis for subsequent management action. As statements of long-range organizational intent and purpose, goals are the ends toward which activity is directed. In a sense, a goal is never completely achieved but rather continues to exist as an ideal state to be attained.
Goals serve as a basis for grouping organizations—for example, educational organizations, healthcare institutions, and philanthropic or fraternal associations. Goals, like statements of philosophy, may be found in an organization’s charter, articles of incorporation, statement of mission, or introduction to the official bylaws. Again, like the statement of philosophy, the overall goals may not bear a specific label and may be identified only through common understanding. The planning process is facilitated when the philosophy and the goals are formally stated. Derivative plans may then be developed in a consistent manner and with less risk of implementing policies and procedures that violate fundamental values.
This overall goal statement for a publicly sponsored rural health agency is an example of the language and style used in stating these plans. This agency has three primary goals:
• To provide services that will enable older adults to maintain a relatively independent lifestyle in both home and community, rather than becoming dependent on institutional care
• To advocate for older adults in the three-county rural area
• To give priority services to those older persons with the greatest social and economic needs
OBJECTIVES
In the planning process, the manager makes the plans progressively more explicit. The move from ideal, relatively intangible statements of mission and purpose or overall goal to the “real” plans is accomplished through the development of specific objectives that bring the goals to a practical, working level. Objectives are relatively tangible, concrete plans and are usually stated in terms of results to be achieved. The manager reviews the underlying purpose and basically answers the question: what is my unit or department to accomplish specifically in light of these overall goals?
Achieving specific objectives tends to be a continuous process; the work of the department must satisfy these objectives over and over again. An overall goal such as “to promote the health and well-being of the community” can be accomplished only through a series of specific objectives that are met on a continuing basis. Objectives add the dimensions of quality, time, accuracy, and priorities to goals. The objectives are specific to each unit or department, whereas the overall goals for an organization remain the same for all units.
Objectives may be stated in a variety of ways, and different levels of detail may be used. For example, objectives may be expressed as follows:
• Quantitatively: to maintain the profit margin of 6% during each fiscal year by an increase in sales volume sufficient to offset increased cost
• Qualitatively: to make effective use of community involvement by the establishment of an advisory committee with a majority of members drawn from the active clients who live in the immediate geographical community
• As services to be offered: to provide comprehensive personal patient care services with full consideration for the elements of good medical care (e.g., accessibility, quality, continuity, efficiency)
• As values to be supported: to ensure privacy and confidentiality in all phases of patient care interaction and documentation
Objectives for the department as a whole may include elements essential for proper delineation of all other objectives. These may be stated as objectives for the organization and need not, therefore, be repeated in the subsequent departmental statement of objectives:
• Compliance with legal, regulatory, and accrediting standards and with institutional bylaws
• Risk management factors, including accuracy
• Privacy and confidentiality in patient care transactions and documentation
• Reference to inpatient as well as outpatient/ambulatory care and other programs sponsored by the organization, such as home care or satellite clinics
Because they are intended to give specificity to overall goals, objectives are the key to management planning. Therefore, objectives must be measurable whenever possible. They must provide for formal accountability in terms of achieving the results. Furthermore, they must be flexible so that they can be adapted to changing circumstances over time.
Two additional planning concepts must be used with the statements of objectives to make them meaningful: the statement of functional objectives and the development of policies. These related plans are both important in fleshing out departmental objectives.
FUNCTIONAL OBJECTIVES
A functional objective is a statement that refines a general objective in terms of:
• The specific service to be provided
• The type of output
• The quantity and/or specificity of output
• The frequency and/or specificity of output
• Accuracy
• Priorities
Some elements, such as accuracy indicators, may be defined for the department or unit as a whole. A general objective’s priority may be implied by its delineation in a related functional objective.
Planning data for organizing and staffing functions may be obtained by inference from statements of objectives. For example, the functional objective statement may include the stipulation that all documentation of patient encounters (e.g., discharge summaries) shall be entered into the electronic health record system. The workload (number of discharge summaries) may be calculated based on the number of discharges per year. A priority system for processing such summaries or a designated turnaround time for such processing provides the necessary parameters for calculating the number of workers needed to meet the objective on a continuing basis. The staffing patterns for day, evening, and night shifts may be developed, again, in a way to satisfy the priority designation and turnaround time contained in the functional objective.
The relationship of the general objective and the functional objectives that support it is clearly seen in the following example, which is drawn from the plans for a transcription/word processing unit of a health information management service.
General Objective: Health information management will provide a system for dictation of selected medical reports by specified healthcare practitioners and for the timely and accurate transcription of these reports on a regular basis.
Functional Objectives: More specifically, this system will provide for:
1. Dictation services for attending medical staff, house officers, and associated professional staff as defined by the medical staff bylaws
2. Transcription/editing of reports will be done within the following time frame:
a. Discharge summaries within 8 hours of receipt of dictation
b. Operative reports within 4 hours of receipt of dictation
c. Consultation reports within 4 hours of receipt of dictation
d. Emergency and priority requests on a “stat” basis
3. Coordination of in-service training for using the system:
a. New employees—at hiring and semiannually thereafter
b. Healthcare practitioners—at hiring and as requested thereafter
4. Maintain quality controls through monthly reviews focusing on accuracy and timeliness of report processing
This example specifies the quantity of output and the time frame and implies the priority of the objective through the designation of the time frame. A statement of accuracy is not included, because it is included in the objectives for the department as a whole. This accuracy statement, which may fall under the overall objective of risk management and quality control, may be expressed as follows:
Health information management strives to carry out its responsibilities and activities with 100% accuracy; therefore, we strive for this level of accuracy.
The following is an example of a general objective and functional objectives from a direct patient care service:
General Objective: The physical therapy department will provide evaluation and assessment procedures appropriate to the patient’s condition as requested by the referring physician.
Functional Objectives: More specifically, this system will provide for:
1. Evaluations within one working day following receipt of the referral.
2. A verbal summary of findings submitted to the physician following the completion of the evaluation.
3. A formal summary of the evaluation entered in the patient’s health record within 8 hours following the verbal report.
POLICIES
Policies are the guides to thought and action by which managers seek to delineate the areas within which decisions will be made and subsequent actions taken. Policies spell out the required, prohibited, or suggested courses of action. The limitations on actions are stated, defined, or, at least, clearly implied. Policies predecide issues and limit actions so that situations that occur repeatedly are handled in the same way. Because policies are intended to be overall guides, their language is customarily broad.
A balance must be achieved when policies are formulated. These comprehensive guides should be sufficiently specific to provide the user with information about the actions to take, the actions to be avoided, and when and how to respond. At the same time, they should be flexible enough to accommodate changing conditions. They should reinforce and be consistent with the overall goals and objectives. In addition, they should conform to legal and accrediting mandates as well as to any other requirement imposed by internal or external authorities. Policies and related procedures have importance in legal proceedings; they constitute the practices identified as those carried out in the normal course of business. For example, in a challenge to the legal chain of custody of evidence, the usual or customary practices, spelled out in policy and procedure, would involve a review of these documents.
Policies are relatively permanent plans, a kind of cornerstone of other, more detailed plans. Yet they must be sufficiently flexible in intent to permit change in the derived plans without necessitating a change in the policy. For example, a commitment to a centralized dictation–transcription/editing system might be made through a policy statement on health information functions. However, no specification is made as to brand of equipment, exclusive use in in-house staffing, or external agency contract. All remain options as long as the equipment selected and the staffing pattern determined meet the policy considerations of an adequate dictation–word processing function. In the dictation–word processing policy, the essential features of the word processing system are delineated. It is easy to derive from this a decision-making matrix for the comparison and selection of one or another commercial transcription–word processing service. In this sense, a policy statement serves to preform or shape detailed decision making because the overall parameters are stated within the policy or are easily derived from it.
Sources of Policy
Department or unit managers develop the policies specific to their assigned areas, but these policies must be consistent with those originated by top management. Policies are sometimes implied, as in a tacit agreement to permit an afternoon coffee break. An implied policy may make it difficult to enforce some other course of action, however, if the implied policy has become standard—in spite of its lack of official approval. Policies are shaped in some instances by the effect of exceptions granted; a series of exceptions may become the basis of a new policy, or at least a revision of an existing one. Certain policies may be imposed by outside groups, such as an accrediting agency or a labor union, through a negotiated contract.
A rich trove of policy and related guidelines is available through national associations of the various health professionals. These associations publish practice briefs and best practice guidelines. These sources reflect state-of-the-art practices, and the wording of these documents is carefully crafted to provide clear guidance. These suggested practices and guidelines are supported by research and field testing.
Another source of wording for policy content is the official publication of a law, regulation, or standard. When these are added to a policy, appropriate citation is made and the excerpt is incorporated with the exact wording of the published law, regulation, or standard.
Wording of Policies
Policies permit and require interpretation. Language indicators, such as “whenever possible” or “as circumstances permit,” are expressions typically used to give policies the flexibility needed. Policy statements in a healthcare institution may concern such items as definitions of categories of patients and designations of responsibility. In a health information service, policy statements may specify, for example, a standardized patient record core content, the use of abbreviations, and the processing of urgent requests.
To decrease the sheer volume of policy statements, a glossary may be developed that includes the institutional definition of “patient” as well as definitions of terms and acronyms referring to members of the medical and professional staff and legal and accrediting bodies. Occasionally, a statement of rationale is included in a policy statement, but the manager should avoid excessive explanations; in general, the manager needs to couch policy directives in wording that predecides issues and permits actions. Another useful adjunct to the complete policy statement is the “Policy in Brief”—a short summary of major points for quick reference.
Policies are somewhat futuristic in that they are meant to remain in force, with little change, for extended periods. In an age of rapid social and technical change, it is helpful to think in broad terms, anticipating change. It also helps to set aside the normal biases that stem from describing the way things are now: increasing use of technology (e.g., telemedicine); expanding scope of practice by physician assistants, nurse practitioners, and technical assistants; and changing levels of care.
Departmental policies typically include these topics:
• Scope of service: list the major functions (e.g., coordination of release of information; maintaining a statistical database)
• Hours of operation and provision for access when department is closed
• Staffing: include a statement that there is a mix of full-time and part-time employees, supplemented by contractual services
• Continuity of operations and succession planning
• Confidentiality, privacy, and data security provisions
• Provision of in-service training
• Participation in education and research
• Risk management and continuous quality improvement
• Interdepartmental coordination
The wording in the following examples, drawn from a variety of settings, tends to be broad and elastic yet gives sufficient information to guide the user. The first example is a policy for the waiver of tuition for senior citizens:
In recognition of their efforts over the years in support of education, the college will waive tuition for academic and continuing education courses for senior citizens who reside in the tricounty area. All residents who are at least 62 years of age and who are not engaged in full-time gainful employment are eligible under this tuition waiver policy. This policy will be subject to annual budgeted funds.
This example provides a general sense of why the college is granting this waiver: in recognition of senior citizen support over the years. The outer limits of its applicability are noted; both academic and continuing education programs are included. A definition of senior citizen is included, and the additional eligibility factors are stated. A final parameter is included to provide flexibility should circumstances change—namely, the limitation determined by the availability of budgeted funds. With this short policy, the necessary procedures can be developed for determining eligibility, and a relatively untrained worker can make the necessary determination.
The following are typical policies for healthcare institutions.
For employee promotion:
It is the policy of this hospital to promote from within the organization whenever qualified employees are available for vacancies. The following factors shall be considered in the selection of individual employees for promotion: length of service with the organization, above-average performance in present position, and special preparation for promotion. Employees on their present job for a reasonable length of time, excluding probationary period, may request promotion during the customary period in which a job is open and posted as being available.
For admission of patients to a research unit:
Because the primary purpose of this unit is research in specialized areas of medicine, the primary consideration in selecting elective patients for admission to the research unit accommodations is given to the teaching and research value of the clinical findings. The research unit offers two types of service: inpatient and outpatient. The research unit reserves the right to assign patients to either service category, depending on the characteristics of the case and facilities available at the time.
For a physical therapy department:
The Physical Therapy Department shall be open from 8:30 A.M. to 4:30 P.M. Monday through Friday and on weekends and holidays as required to meet patient care needs.
The following is an example of a policy regarding professional credentials:
All occupational therapy personnel will be licensed and registered.
Each applicant will submit the names of two references, and the human resources officer will contact these individuals and check on the applicant’s ability to problem solve and communicate with others and his or her work habits and commitment to patient service delivery.
The director of the occupational therapy department will check to see if the applicant has passed the national certification examination and has a current state license.
Recent graduates or therapists from foreign countries may treat patients but they must be supervised by a licensed and certified occupational therapist who reviews their patient care plans and progress notes.
Occupational therapists may not work more than 6 months under these conditions. If not registered and licensed within 6 months after hire, employment must be terminated.
PROCEDURES
A procedure is a guide to action. It is a series of related tasks, listed in chronological order, that constitute the prescribed manner of performing the work. Essential information in any procedure includes the specific tasks that must be done, at what time or under what circumstances they must be done, and who (job title, not name of employee) is to do them. Procedures are developed for repetitive work to ensure uniformity of practice, to facilitate personnel training, and to permit the development of controls and checks in the workflow. Unlike policies, which are more general, procedures are highly specific and need little, if any, interpretation.
Procedures for a specific organizational unit are developed by the manager of that unit. As with other plans, departmental procedures must be coordinated with those of related departments as well as with those developed by higher management levels for all departments. For example, the procedures for patient transport to various specialized service units, such as nuclear medicine, physical therapy, or occupational therapy, are developed jointly by the nursing service and these related departments or services. In contrast, procedures relating to employee matters may well be dictated by top-level management for the organization as a whole with little, if any, procedural development done at the departmental or unit level.
Procedure Manual Format
There are two common format types used in procedure manuals: narrative and abbreviated narrative. The narrative format contains a series of statements in paragraph form, with special notes or explanations in subparagraphs or in footnotes. This format has the disadvantage of being difficult to refer to quickly and easily. The abbreviated narrative format illustrates procedures through the use of key steps and key points (Exhibits 5–3, 5–4, and 5–5). When a procedure involves several workers or departments, it is useful to identify each participant by job title. The step is given a sequence number, key action words are stated, and action sentences are developed for the step (see Exhibit 5–5)
EXHIBIT 5–3 Abbreviated Narrative Procedure Format: Procedure for Terminal Digit Filing
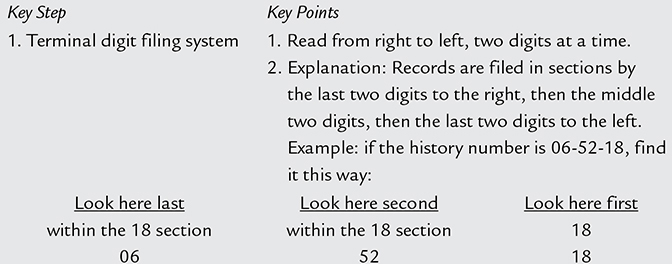
Look here second within the 18 section 52
EXHIBIT 5–4 Abbreviated Narrative Procedure Format: Procedure for Interdepartmental Coordination
| Key Step | Key Points |
| 1. Determine patient care need. | 1. Review medical care record. 2. Perform appropriate evaluation procedures. 3. Complete related medical documentation, including information needed for consultation. |
| Key Step | Key Points |
| 2. Contact appropriate department. | 1. Make verbal contact via telephone. 2. Confirm through interdepartmental request form for joint conference. |
The physical format of the procedure manual is important. A procedure manual should be convenient in size, easy to read, and arranged logically. If the manual is too large or too heavy for everyday use or is difficult to read because of too many unbroken pages of type, workers tend to develop their own procedures rather than referring to the manual for the prescribed steps. The choice of a format that makes it easy to update the manual (e.g., loose-leaf binder) removes a major disadvantage or limitation regarding the manual’s use—pages of obsolete procedures. The use of electronic media is, of course, a convenient option.
Development of the Procedure Manual
The manager who is developing a procedure manual must first determine its purpose and audience (e.g., to train new employees or to bring about uniformity of practice among current employees). The level of detail and the number and kinds of examples depend on the purpose and the audience. Clarity, brevity, and the use of simple commands or direct language improve comprehension. Action verbs that specify actions the worker must take help to clarify the instructions. Keeping the focus of the procedure specific and its scope limited permits the manager to develop a highly detailed description of the steps to be followed. The steps are listed in logical sequence, with definitions, examples, and illustrations.
Methods improvement is a prerequisite for efficient, effective procedure development. Flow charts and flow process charts are useful adjuncts to the procedure manual because they require logical sequencing and make it possible to reduce the backtracking and bottlenecks in the workflow.
EXHIBIT 5–5 Examples of Key Steps and Detailed Steps

METHODS
The way in which each step of a procedure is to be performed is a method. Methods focus on such elements as the arrangement of the work area, the use of certain forms, or the operation of specific equipment. A method describes the preferred way of performing a task. The manager may develop methods detail as part of the training package for employee development, leaving the procedure manual free of such detail.
RULES
One of the simplest and most direct types of plan is a rule. A continuing or repeat-use plan, a rule delineates a required or prohibited course of action. The purpose of rules is to predecide issues and specify the required course of action authoritatively and officially.
Like policies, rules guide thinking and channel behavior. Rules, however, are more precise and specific than policies and, technically, allow no discretion in their application. As a result, management must direct careful attention to the number of rules and their intent. If the management intent is to guide and direct behavior rather than require or prohibit certain actions, the rule in effect becomes a policy and should be issued as such.
Like procedures, rules guide action; unlike procedures, however, rules have no time sequence or chronology. Some rules are contained in procedures (e.g., “Extinguish all smoking material before entering this facility”). Other rules are independent of any procedure and stand alone (e.g., “No smoking”). The wording of rules is direct and specific, such as:
• Food removed from the cafeteria must be in covered containers.
• Books returned to the library after 4:00 P.M. will be considered as returned the following day, and a late fine will be charged.
• Children younger than the age of 12 must be accompanied at all times by an adult who is responsible for their conduct.
PROJECT PLANNING
In addition to developing the operational plans for day-to-day functioning, managers sometimes undertake intensive project planning for major initiatives. Examples include:
• Implement an organization-wide electronic health record over a 4-year period.
• Form a regional health information exchange over a 2-year period.
• Enhance the revenue cycle processes to maximize reimbursement by collecting all the revenues to which the organization is entitled. To accomplish this in a timely manner, systems and workflow changes are to be implemented during the first 3 months of the new fiscal year.
• Develop a leadership succession plan for the next 3 years in anticipation of planned retirement of (n) executive-level managers.
Extensive projects, such as planning and opening a new service, developing an educational division, or expanding an existing program to include satellite facilities, generally fall under the rubric of major project planning.
A major project reflects the elements of general planning (e.g., assumptions, constraints, goals and objectives, timeline). Project planning is sometimes expressed primarily in terms of time frame, as in a 500-day plan to gain momentum and to demonstrate major achievements. In the 500-day plan, a rolling cycle of designated periods is delineated (e.g., 90 days, 100 days, 13 weeks), with adjustments to the plan made at the conclusion of each phase. The designated periods are not necessarily the same for each activity. As one phase is completed, an additional phase is added until the rollout of the project has occurred. Planning for the next phase is fine-tuned in light of the outcomes in the preceding period. The goals for such initiatives reflect actions that have the potential to yield the most results. For example, a fetal alcohol syndrome disorders clinic might focus on early intervention through emphasis on prenatal care. Other aspects of the program simultaneously unfold, but the major focus is this aspect of care.
The Project Manager
The project manager is the designated coordinator of the planning and execution of the project. For large, organization-wide projects, this manager may hold an executive level position. For projects within a division or department, the middle manager might take on that role, or he or she might delegate it to an assistant who has authority and responsibility over the system that is the focus of the project. Sometimes an outside consultant is hired as the project manager as in the case of new products, systems, and equipment. This individual would have knowledge of the new system, along with expertise in implementation. Colleges and universities, along with private organizations, offer training and certification in project management. Professional organizations offer similar programs, tailored to the interests and needs of the particular profession.
ELEMENTS AND EXAMPLES OF MAJOR PROJECTS
At the outset of developing a major project, the project manager and team decide on the desired level of detail of the plan. In general, a major project includes the customary elements, described here, with some examples of wording. Exhibit 5–6 provides a more detailed example of the project elements, timelines, and wording of a major project plan with a 500-day timetable.
Name of Project
This should be precise but informative, as in Developing and Implementing a Neighborhood Health Center in the Northeast Catchment Area of the City of Clarion.
Focus and Scope of the Project
This section provides an overview of the project. Specify whether the project is a new one or an extension of an existing project. Provide brief background information. Has funding been obtained? Have feasibility studies completed? Sample wording of focus and scope might be:
This new project has as its focus the development and implementation of a comprehensive neighborhood health center in catchment area 25 of Clarion City’s master health plan. The projected time line is augmented by a detailed timeline and milestone event listing included in the body of this proposal. The overall timeline is:
• January 1, year one: Development phase
• July 1, year one: Phase One—limited opening of clinic for maternal and infant care as well as school-age youth care
• October 1, year one: Phase Two—opening of all the remaining clinics; programs fully operational
• July 1, year two: Transition from grant funding to freestanding, community-sponsored clinic, with 6-month transition funding (July–December)
• January 1, year three: Transition funding ends; clinic is self-supporting
Scope of Service
The clinic is a primary care facility, with as-needed referrals to a tertiary care hospital and specialty clinics. It deals with ambulatory care—scheduled, walk-in, or urgent.
The target population include mothers and infants, preschool and school-age children and youth, and adults. There is a special emphasis on homeless youths and adults. (The target population figures/planned numbers would be given here.)
Project Manager and Project Team
Key personnel are identified, with a listing of name, title, and organizational authority/responsibility. For example:
The Project Manager is Dr. Leslie H. Deal, Associate Vice President for Community Outreach, Clarion Health Systems. Project Manager Associates are the designated representatives from the direct patient care and support services staff. (A list of names and titles would be given here.) These associates report directly to the project manager, who, in turn, reports to the Vice President for Community Outreach, Clarion Health Systems.
Time Frame and Milestone Events
The time frame provided in the opening section on the focus and scope of the project is repeated and amplified in this section. Managers develop a level of detail best suited to the project and their management style. If time is critical, with little or no leeway, and/or if there are multiple contingent activities, the timeline is detailed and precise. For example, time specifications could include three estimated time calculations: the probable, most likely (realistic considerations noted); the pessimistic (if everything or many things go wrong); and the optimistic (everything goes as scheduled, no equipment breakdowns, no staff turnover, no delay in obtaining material). The beginning and ending time frame for each activity is specified.
Milestone events are listed. These are the markers for major accomplishments, such as completion of equipment selection, completion of site renovations, and accomplishment of an immunization and physical examination program for preschool children.
Activities are carried out to lead to the completion of a milestone or landmark event. For example, developing a job analysis, job descriptions, and a wage and salary scale for clerical and technical support staff leads to the milestone of completion of foundational analysis and description of clerical and technical support staff documents. Note: Activities and events are not solely sequential; some activities, and therefore the accomplishment of events, may occur simultaneously.
Cost Factors
Project managers develop a related tracking process for budgeting; the monitoring timeline is associated closely with the step-by-step implementation. This financial monitoring and auditing can be built into the evaluation process.
The Evaluation Process
Both public and private organizations require sound evaluation processes. The federal government’s Program Evaluation for Effectiveness Review is one example of detailed evaluation requirements. Program evaluation focuses on the systematic collecting, evaluating, and using information to answer the basic question. Did the program accomplish what it set out to do? Did the program meet its proposed goals?
There are two categories of evaluation: process and outcome. Process evaluation focuses on the start-up activities that need to be in place before direct services can be offered (e.g., site location secured, physical renovations completed, license to operate obtained). In addition to a major process review at the end of the development phase of the project, ongoing process review occurs throughout the life of the project to ensure smooth operations. For example, in a project with limited service offerings, followed by full-scale service offerings, particular attention would be given to the functionality of the systems when the program is expanded. Evaluation methods could include sampling of workflow, equipment, error rates, turnaround times, flow of intake, and registration process.
Outcome evaluation focuses on the results in terms of effect on target population. Did the project reach the intended numbers and categories of patients? Factual data are presented. For example, data for a social service project might show:

A short narrative explanation of reasons for overprojection or underprojection would be included.
If the project focus includes behavior changes in patients, these would be reported (e.g., successful smoking cessation rates, wellness behaviors). Client satisfaction with services is another indicator of program success. (Interviews and surveys are the source of this information.)
The sources of information about patient care outcomes include studies drawn from documented care, patient satisfaction surveys, aggregate data about infection rates, patterns of “no-show” appointments or noncompliance, and number of return visits. If there are unexpected results, these are explained in detail. For example, the need for coordination of transportation from clinic to tertiary hospital’s clinics might surface. Or the planned focus on school-age at-risk youth might have changed to a wider focus to include at-risk youth who no longer attend school.
The evaluation process properly includes both internal and external review, along with appropriate intervals of review. One final review is insufficient to make course adjustment. The internal review and its time frames are developed to correspond with milestone events (e.g., frequent reviews during development phase to ensure on-time opening of a clinic). These reviews are internal for the most part. An outside peer review, perhaps from the affiliated health system, would usually be invited because the systems of the two organizations need coordination. External review teams include the peer review, as noted, along with coaching reviews by accrediting agencies, external financial audit, or community boards.
Exhibit 5–6 provides excerpts from a major project, coupled with the 500-day planning approach. See also Chapter 12 of this text on strategic planning and related examples.
THE PLAN AND THE PROCESS
Referring back to the beginning of the chapter, it is perhaps pertinent to offer a reminder that planning always involves tentatively deciding what might be done in a time period that is not yet here—that is, at some point anywhere from the very near to the far distant future. People plan because they do not know for certain what changes will occur in the environment; they plan because every decision carries with it some elements of risk and uncertainty.
Of course, the environment will change between the time people make their tentative decisions and the time the future becomes the present, and of course they enter the overall process with less-than-perfect information about not only what the future will bring but often also what the present contains. Because change is continual and only partially predictable, people know at the outset that rarely will their plans be fulfilled exactly as planned. This does not, however, mean that planning is a futile activity. On the contrary, it means all the more than might be suspected that planning is essential.
In and of themselves, plans—those collections of stated targets with dates and desired results attached—are not especially valuable. What is of inestimable value is the planning process, that cycle of activities in which people gather information, tentatively decide what is to be done and do it, monitor progress, alter methods as the environment changes and the unforeseen occurs, modify targets as necessary, and go through it all over again but differently. Even if the stated target remains fixed and valid but not attained, the simple presence of the target provides information people would not have had without it—they know by how much they missed, and thus they know how much they must correct their approach for the next attempt.
EXHIBIT 5–6 Project Plan for Neighborhood Health Center with 500-Day Timeline
(Note: This exhibit shows excerpts from the project plan to illustrate the usual content and wording. There would be several supplementary attachments, such as budget and audit protocols.)
Name of Project
Development and Implementation of a Neighborhood Health Center in the Northeast Catchment Area of the City of Clarion
Focus and Scope of the Project
This new project has as its focus the development and implantation of a neighborhood health center (NHC) in catchment area 25 of Clarion City’s master health plan. The health center’s services will be coordinated with the city health department clinic and the outpatient clinics of the University Hospital’s tertiary care center. A combination of a federal grant and private funding has been secured by the University Hospital for the first 2 years of operation. A plan for transition to freestanding status has been developed. The grant application, including feasibility study and related background information, is attached.
A full range of services will be offered. There will be primary care, with as-needed referrals to the University Hospital tertiary care hospital and its clinics. Ambulatory care will include both scheduled and walk-in routine and urgent care services. The target populations is a mix of adult and children. Initial emphasis will be given to maternal and infant care and young child care (preschool children and children in primary grades). Then the scope of service will be expanded to older children and adults. Special emphasis will be given to homeless youth and adult populations.
Overall Time Frame
| January 1, 20×1–June 30, 20×1 | Preliminary development phase |
| July 1, 20×1–September 30, 20×1 | Phase One of clinic service: maternal and infant care, young child care (preschool children and children in primary grades) |
| October 1, 20×1–November 30, 20×1 | Phase Two of clinic service: general population (youths and adults); clinic fully operational |
| December 1, 20×1–December 31, 20×1 | Phase Three: outreach program begun for homeless (both youth and adult) |
| July 1, 20×2–December 31, 20×2 | Transition phase from University Hospital sponsorship to freestanding neighborhood center, under sponsorship and control of community agency |
| January 2, 20×3 | Independent, freestanding neighborhood center fully operational, with 2-month transitional funding from grant obtained by community agency |
| March 1, 20×3 | Fully self-sustaining clinic |
(A detailed timeline, with key events, is attached.) The 500-day pattern of planning cycles reflects 100-day cycles, with the rolling addition of 100-day cycles as each planned cycle is completed.
Project Manager and Project Team
The Project Manager is Dr. Leslie H. Deal, Associate Vice President for Community Outreach, University Hospital. Project Manager Associates are the designated representatives from the direct patient care staff and administrative support services of the hospital. (A complete list of names, titles, and responsibilities is attached.) The associate project managers report directly to the project manager who, in turn, reports to the Vice President for Community Outreach, University Hospital.
Cost Factors and Tracking
The generally accepted financial practices will be followed. This includes a monthly internal audit by the finance department of University Hospital; special oversight review and audit by the Vice President for Community Outreach to conform to grant funding requirements. A quarterly audit by an independent auditing firm augment the internal audits. (Sample audit protocols are attached.)
Evaluation
Both internal and external evaluation processes have been developed. Evaluations will be done throughout each phase of the project. Their frequency varies from 1 month to 6 weeks to quarterly, depending on the focus of the review. Process evaluation methods will be used for administrative activities. Outcome evaluation methods will be used to reflect patient care and client and community-at-large satisfaction with clinic services. (A detailed listing of the timeline and evaluation methods is attached.)
Evaluators include internal review committees and teams and external, independent reviews, including peer teams from the sponsoring hospital and its related university, as well as peer professionals from clinics in the region. An independent review will be carried out by a designated accrediting agency that provides preliminary coaching reviews for outpatient services.
Detailed Timeline of Activities: 500-day plan (excerpts)
Cycle One: 100 days (January 1, 20×1–April 10, 20×1)
January
• Incorporation filed; state agency approval to operate received
• Physical site secured; renovations begun
• Administrative processes developed
• Mission; goals and objectives; policies; procedures
• Staffing patterns developed
• Monthly budget review and reconciliation completed by NHC staff
(This review will be done every month and would be listed as an activity and related event for each month using this same wording.)
February
• Neighborhood community board configured and members selected and oriented
• Collaborative arrangements completed for mutual referrals (University Hospital, city health department clinics, local schools—prekindergarten and primary grades)
• Monthly budget review of previous month completed
• Process evaluation completed by peer review team from University Hospital and NHC staff
• Process evaluation completed regarding legal, regulatory, corporate compliance (carried out by Vice President for Corporate Compliance and Chief Development Officer of University Hospital)
• Patient care practitioners and administrative support staff recruited for Phase One: program opening (for July 1)
March
• Equipment selected, received, and debugged
• Quarterly external financial audit and budget review completed
• Pilot run completed (intake and registration; flow of patient care through care site)
• Peer group review of administrative and patient care processes completed by NHC staff and University Hospital clinic counterparts
April
• Direct patient care staff and administrative support staff recruited for Phase Two of clinic operations (scheduled for late October)
• Quarterly financial audit completed by external auditors
• Process evaluation of administrative functions completed by NHC staff
Cycle Two: 100 days (April 11, 20×1–July 19, 20×1)
April
• Outreach to community completed (detailed outreach plan is attached)
May
• All hiring and orientation completed
• All requirements met regarding billing Medicare, Medicaid, and city health agency
June
• Pilot run completed: sampling of patient population recruited and treated (200 maternal and infant care patients, 50 prekindergarten children)
• Final review of administrative and patient care processes completed
July 1
• NHC officially opened
Cycle Three: 100 days (July 20, 20×1–October 28, 20×1)
July
• Evaluation of outreach program completed by NHC staff
August
• Outreach program completed (youth and adults for Phase Two)
• Outreach program evaluation completed (NHC staff, community board, representatives from local schools)
September
• Outcome evaluations completed for maternal and infant care and prekindergarten care
• Additional staff for Phase Three hired and oriented (social worker and nurse practitioner)
• Outreach program for Phase Two completed (general population)
• Process review of intake and care flow completed (maternal and infant care and prekindergarten care)
• Patient satisfaction information captured and compiled (maternal and infant care)
October
• Phase Two programs opened (general population)
• Agreements with nonprofit Host Home Program for at-risk youths completed
• Agreements with local homeless shelters (referrals) completed
• Quarterly external financial audit completed
Cycle Four: 100 days (October 29, 20×1–February 5, 20×2)
November
• Transportation needs survey completed and analyzed
• Community Board input and review of transportation needs completed
• Action plan developed:
○ Donation of van obtained
○ Schedule of transportation to and from University Hospital specialty clinics developed
○ Van driver hired ($10.00/hour for 8-hour day Monday through Friday)
○ Budget allocations reassigned to cover driver’s wages and fringe benefits; money taken from training budget and from refurbishing funds for 20×2; arrangements made for free training by University faculty as an in-kind donation
December
• Homeless and at-risk youths outreach extended to youths not attending school (street outreach, soup kitchen, emergency winter shelters in catchment area [four overnight shelters, two day shelters])
• Coordination of shelter services with partnering agencies completed (focus on homeless adults)
• Coordination of services, and referral processes completed (community mental health agencies for adults; clean and sober programs for adults)
• Process survey completed (focus on patient/client satisfaction with transportation and with intake-care flow)
• Peer review completed
○ Focus on administrative processes: regional peers
○ Focus on direct care provision: regional peers
January
• Quarterly external financial audit completed
• Internal review completed: billing compliance (review team coordinated by Vice President for Compliance and Chief Financial Officer of University Hospital)
• Patient care outcomes review completed (focus on wellness and immunizations; medication compliance; patterns of care: chronic conditions of diabetes, obesity, and blood pressure)
February
• Process evaluation: review of transportation services completed
Cycle Five: 100 days (February 6–May 17, 20×2)
February
• Repeat patient care outcomes evaluations completed; comparison study completed
March
• External regional peer review completed (focus on administrative processes and outcomes, with emphasis on data from comparison studies)
April
• Quarterly external financial audit completed
• Community agency, nonprofit corporation formed
• Preliminary plans for transition in 20×3 begun
• Outcomes review completed: community-at-large survey
May
• Transitional funding request for 20×3 completed and submitted to city’s Community Development Fund
May 17, 20×2 END OF FIRST 500-DAY CYCLE
Cycle Six: 100 days (May 18, 20×2–August 26, 20×2)
(activities and events reflecting ongoing operations)
Cycle Seven: 100 days (August 27, 20×2–December 5, 20×2)
August (activities and events reflecting ongoing operations)
September
• External funding for transition received
October
• Quarterly external financial audit completed
• Billing compliance internal review completed
• Additional administrative processes implemented regarding incomplete and late billing
• Preliminary close out for line items in budget completed
• Revenue projections for 20×3 completed
November
• Transition plan completed
December 5
• Transition plan implemented
Cycle Eight: 100 days (December 6, 20×2–March 16, 20×3)
December
• Process review of all administrative systems completed
• Outcomes review of patient care (all categories) completed
• Due Diligence Review completed
• December 31, 20×2:
○ Official end of University Hospital sponsorship
○ End of 2-year funding grant
January 1
• New funding cycle (transitional funds) begun
February
• Detailed plan for self-sufficiency funding developed and implemented
• Final audit of 2-year University Hospital funding completed (reflecting late charges and final billing as well as closeout of budget line items)
March 16
• Transitional funding completed; clinic is fully self-sustaining
Giving special attention to the decision-making phase may be a useful adjunct to this phase of planning.
DECISION MAKING
Evaluating a Decision’s Importance
By its nature, decision making means commitment. The importance of a decision may be measured in terms of both the resources and the time being committed. Some decisions affect only small segments of the organization, whereas others involve the entire organization. Some decisions are irrevocable because they create new situations. The degree of flexibility that remains after the commitment has been made may also be used when evaluating the significance of a decision. Are the resulting conditions tightly circumscribed, with little flexibility permitted, or are several options still available in developing subsequent plans? Decisions regarding capital expenditures, major procedural systems, and the cost of the equipment that must be prorated over the projected life of the equipment are examples.
The degree of uncertainty—and therefore the degree of risk—associated with a decision is another dimension that must be evaluated in weighing its impact. The greater the impact in terms of time, resources, and degree of risk, the more time, money, and effort that must be directed toward making such decisions. Uncertainty is caused, in part, by a lack of necessary information or the impossibility obtaining comprehensive, reliable data. The consequence of some events may not be known until an action or a project has been undertaken and sufficient information is generated to make additional plans.
The management team must proceed in some instances without full certainty. There are costs associated with inaction and indecision. For example, the opportunity to expand a program, to increase client base, or to obtain special funding may be lost if timely action is not taken. Other aspects of inability to make decisions, which have associated costs and impacts, include:
• Failure or delay in making necessary capital improvements, resulting in (1) increased safety hazards for clients and workers and (2) greater costs due to deterioration of physical plant
• Loss of licensure or accreditation because of failure to meet standards
• Decrease in client perception of the organization’s quality, causing clients to seek service elsewhere
Therefore, the management team attends to decision making, even in the face of uncertainty. The team uses such strategies as incremental implementation, taking advantage of the unfolding dynamic in which unknowns become knowns; thus, uncertainties become clearer, and plans can be revised.
Finally, in any organization, effects of a decision on humans are a major factor. The environmental impact and social costs must be assessed. Decisions have a cascading impact—sometimes positive, sometimes negative. In the planning–decision phase, managers anticipate second- and third-order effects: the desired outcome is the first cause–effect dyad. This, in turn, causes a second-order effect, which leads to a third-order effect. By way of example: consider the decision by a healthcare team to open an outreach, walk-in clinic in a busy, congested neighborhood. This is done with the positive result of easier access by clients to the care they desire. As the client usage rises, so does the traffic and related parking congestion; this second-order effect is a negative one, with both merchants and residents becoming disaffected with the clinic. They, in turn, begin to boycott the clinic and call for increasing inspection and regulation of the facility; this is a third-order event.
Managers try to anticipate second- and third-order effects in order to prevent or mitigate them. Managers seek to avoid unanticipated consequences, as for example, the efficient regrouping of transportation for frail, elderly people in a continuing care facility. In one instance, instead of picking up one person at a time, designated pick-up stations were set up. This resulted in more falls and accidents in inclement weather, causing obvious harm to the clients, and an increase in lawsuits for negligence. Originally, the cost-savings idea had seemed like a good one, but the reality reflected a different result. Both positive and negative factors influence the process by which alternatives are evaluated.
Evaluation of Alternatives
To evaluate alternatives, a manager must adopt an underlying philosophical stance and make a preliminary decision about the approach to decision making that will be taken. Depending on this philosophical stance, certain alternatives will be considered acceptable, and others will be excluded automatically. Root and branch decision making, satisficing, maximizing, and the use of Paretian optimality are among the fundamental types of (or approaches to) decision making that partially determine the decisions that are actually reached.
Root and Branch Decision Making
Certain decisions are so basic to the organization’s nature that their effects are pervasive and far-reaching in terms of organizational values, philosophy, goals, and overall policies. Such decisions—termed root decisions—invest the organization with its fundamental nature at its inception and carry it through periodic, comprehensive reviews of its fundamental purpose, often resulting in massive innovation. Thus, in the life cycle of an organization, root decisions may be associated with gestation, when the fundamental form and purpose of the organization are crystallized. They may also occur in middle age, when new goals are developed and new organizational patterns are adopted. Finally, during old age and decline, a fundamen
tal decision to dissolve the organization may be made.
The pervasive effect of root decisions may be seen in the decision of a board of trustees to change a 2-year college into a baccalaureate degree–granting institution or to convert a hospital into a multicomponent healthcare center. Consider the decision made by a health information administrator who chooses to use off-site commercial storage for hard copy records. When this change is implemented, the existing space for hard copy records will be eliminated and will not easily be recovered. Policies and procedures, budget considerations, and changes in staffing patterns also result. Such a decision has long-lasting implications. For these reasons, it ranks as a root decision.
Other examples of root decisions can be found in the major changes made by some professional associations, such as the AHIMA’s decision to open active membership to all who are interested in the primary work of this organization. Another example of such change is the American Physical Therapy Association’s decision to emphasize doctoral-level preparation as the norm for its practitioners.
Charles Lindblom described root decisions and their opposite, branch or incremental decisions.2 According to Lindblom, these incremental, limited, successive decisions do not involve a reevaluation of goals, policies, or underlying philosophy. Rather, objectives and goals are recycled and policies are accepted without massive review and revision. Change occurs by degree, and only a small segment of the organization is affected.
Branch decision making is more conservative in its approach than is root decision making, with innovation being inhibited during the former. The stability of organizational life is enhanced, in many cases, when decision making is of the successive, incremental type, because the manager does not have the option of completely reviewing the organizational structure, functions, staffing patterns, equipment selection, and similar capital expenditures. Incrementalism also simplifies decision making because it tends to limit conflicts that might occur if the patterns of compromise, consensus, organizational territory, and subtle internal politics are disturbed. Moreover, incrementalism may be the simple outcome of previous root decisions. However, the manager may overlook some excellent alternatives because they are not readily apparent in the chain of successive decisions. Incrementalism lacks the built-in safeguard of explicit, programmed review of values and philosophy.
Satisficing and Maximizing
“It might easily happen that what is second best is best, actually, because that which is actually best may be out of the question.” This quotation, attributed to the philosopher–educator Cardinal Newman, expresses the idea contained in the concepts of satisficing and maximizing. In decision making, the one best solution may be determined by developing a set of criteria against which all alternatives are compared until one solution emerges as clearly preeminent. In the form of decision making known as maximizing, this one best solution is the only acceptable one.
In the form of decision making known as satisficing (a term used by Simon3), a set of minimal criteria is developed, and any alternative that fulfills those criteria is considered acceptable. A course of action that is “good enough” is selected, with the conscious recognition that better solutions may exist. When the manager seeks several options, satisficing may be employed. Like incrementalism, satisficing obstructs absolute, rational, optimal decision making, yet it simplifies the process. In satisficing, the manager accepts the fact that not every decision need be made with the same degree of intensity.
The Pareto Principle (Paretian Optimality)
Vilfredo Pareto (1848–1923) was an Italian economist and sociologist who postulated a criterion for decision making that is referred to as the Pareto principle or Paretian optimality.4 He suggested that each person’s needs be met as much as possible without any loss to another person. In this mode of decision making, certain alternatives are rejected because they would produce a decrease in benefits for one or several groups. Decisions that result in a major gain for one individual with a concomitant major loss for another are avoided. This approach involves compromise and consensus, with each manager accepting the needs of other units of the organization as legitimate and the needs of the organization as a whole as paramount. The concessions and trade-offs in the budget process or in the labor negotiation process illustrate the balance required to satisfy the needs of many departments or groups without penalizing any one of them (or by penalizing all departments or groups in equal measure if penalties are unavoidable).
Continuing Assessment of Decisions
The decision-making process includes continuous analysis of decisions. Through the feedback process, a new agenda is generated and new alternatives are revealed. The steps in the control process provide a link back to the planning and decision-making functions. This feedback process necessarily pervades organizational life. Planned, formal review is built into operational plans and decisions such as budget preparation, accrediting self-study processes, and labor union contract review. In addition, there is need for continuous real-time assessment of decisions that require rapid response to changing situations. An example of such a condition is an outbreak of an epidemic; disruption of service because of a protracted and polarizing labor strike is another such circumstance.
In this type of situation, the classic OODA loop, or Boyd cycle, provides a method of rapid assessment and real-time adjustments to the pressing situation. This strategy was developed by Colonel John Boyd of the U.S. Air Force (retired) and has been widely used in military operations.5 Businesses have adopted the general schematics of the OODA loop in responding to rapid change in their own and their competitors’ environment. OODA is the acronym for:
• Observe: the fact-gathering stage, which emphasizes the immediate situation and its changed reality
• Orient: an assessment of one’s own position in relation to the changed situation
• Decide: a rapid decision to commit to a new course of action in light of the changed circumstances
• Action: implementation of the new course of action immediately, without delay
The use of the OODA loop is predicated on managerial flexibility and a high degree of delegation of authority. This decision-making process is intended for use in the field by highly skilled professionals who need to act without continual reference back to some other authority. Rapid adjustment to the plans is a key characteristic.
The after-action report (AAR) or “hotwash” review is a method used in emergency response–disaster management. As soon as possible after the crisis has been dealt with, but before the response team leaves, a rapid review is completed—what worked, what did not, and what situations need further review. For example, on the “plus” side, there may have been rapid and coordinated response of two or more local service units and available supplies and personnel when surge capacity needed increasing. On the “minus” side, there also may have been portable lighting on scene that was insufficient, traffic diversion that needed to be accomplished earlier, and radio frequencies that required recalibration. Using AARs, a lessons-learned session may be held at a later date to consolidate the findings and make recommendations.
DECISION-MAKING TOOLS AND TECHNIQUES
Managers have available a variety of historical records, information about past performance, and summaries of their own and other managers’ experience. In addition, managers may test alternatives through the use of decision-making tools and techniques.
Considered Opinion and Devil’s Advocate
A manager may obtain the considered opinion of experts and use the technique of the “devil’s advocate” to sharpen the arguments for and against an alternative. In the first instance, the manager asks staff experts or other members of the management team to assess the several alternatives and develop arguments for and against each. The resulting comparative assessment helps the decision maker to select a course of action.
When the devil’s advocate technique is used, the decision maker assigns an individual or group the duty of developing statements of all the negative aspects or weaknesses of each alternative. Each alternative is then tested through frank discussion of weaknesses and errors before the final decision is made. The underlying theory is that it is better to subject alternatives to strict, internal, organized criticism than to run the risk of having a hidden weakness or error exposed after a decision has been implemented. The devil’s advocate does not make the decision but simply develops arguments to ensure that all aspects are considered.
The Factor Analysis Matrix
For the decision maker who must overcome personal preference to make an impartial decision, the matrix of comparative factors is an effective tool of analysis. As a first step, the decision maker develops the criteria under two major categories: essential elements (musts) and desired elements (wants). The manager begins this process by listing key factors relating to the topic. For example, in weighing alternatives to select an outsourcing service for dictation–transcription functions, the manager would consider the following points:
• Health Insurance Portability and Accountability Act (HIPAA)-compliant encryption
• Accepts dictation from landline phone systems and personal digital assistant devices
• Document distribution system by secure e-mail and remote print
• Electronic edit and authentication
• One-screen tracking of documentation from beginning of recording through the finished document received at the client site
• Temporary or total outsourcing services for seasonal peak loads
• Customized formatting
• STAT capability
• 24-hour/365-day support center
• Turnaround time of 12 hours for routine reports
• Conformity with standardized billing method principles
• Zero capital investment on site: use of standard Internet connections
The choices available are compared by developing a table or matrix. The factors can be assigned relative weights, as in a point scale, with the alternative with the highest point value becoming the best option. Even without the weighting factors, the matrix remains useful as a technique of factual comparison. Table 5–1 illustrates the use of the “must” and “want” categories to compare equipment for departmental use. A similar process could be used to evaluate applicants for a job; personal bias can be set aside more easily and candidates compared on the basis of their qualifications for the position (Table 5–2).
The Decision Tree
A managerial tool used to depict the possible directions that actions might take from various decision points, the decision tree forces the manager to ask the “what then” questions (i.e., to anticipate outcomes). Possible events are included, with a notation about the probabilities associated with each. The basic decisions are stated, with all the unfolding, probable events branching out from them. Decision trees enable managers to undertake disciplined speculation about the consequences, including the unpleasant or negative ones, of actions. Through the use of decision trees, managers are forced to delineate their reasoning, and the constraints imposed by probable future events on subsequent decisions become evident. Each decision tree reveals the probable new situation that results from a decision.
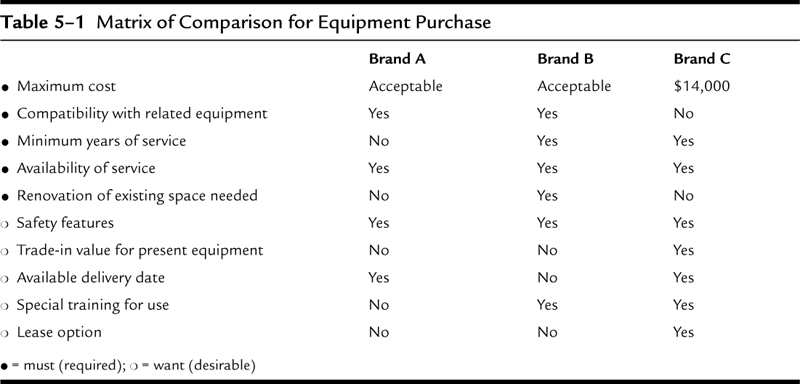
It is possible to use a decision tree without including mathematical calculations of probability, although computers are commonly used to calculate the probability of events when such detailed information is available. Managers in business corporations with sufficient market data about profit, loss, patterns of consumer response, and national economic fluctuations include these data in the construction of a decision tree for the marketing of a new product, for example.
Managers who lack detailed information of this type can still use decision trees to advantage. In developing decision trees, these managers use symbols to designate points of certainty and uncertainty. For example, events of certainty may be placed in rectangles; events of uncertainty in ovals. This technique emphasizes the relative risk in each decision track. The goal to be reached is the continual reference point. The sequence of decisions that leads to the goal with the least uncertainty emerges as a distinct track, thereby facilitating the manager’s decision. For decisions in which the manager has intense personal involvement, this approach is a valuable aid in overcoming emotional barriers to objective choice.
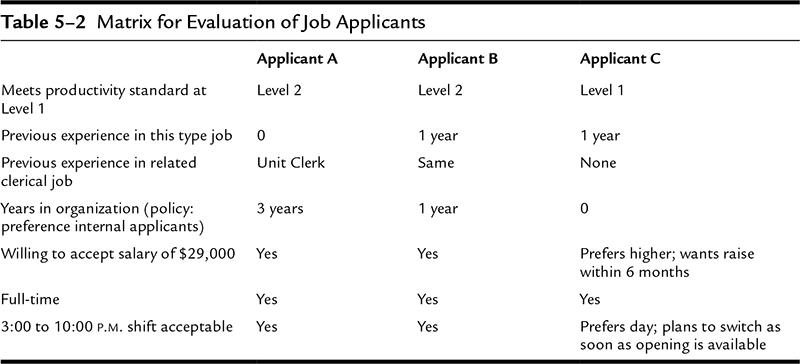
When managers devote time and effort to sound decision making, the planning process is enhanced, leading to consistent achievement of organizational goals.
EXERCISE: FROM INTENT TO ACTION: THE PLANNING PATH
Select a specific healthcare organization that you know something about. If you are or have been employed in health care, use your employing organization. (Whether the example consists of your organization or another, there is no need to specifically identify it.) You may use a hospital, nursing home, health center, rehabilitation service, surgicenter, urgent care center, or any of a number of other health settings. Assume you are a department manager within your chosen setting.
For your chosen organization:
1. Write a mission statement for the organization—a concise yet appropriately descriptive of why the organization exists.
2. Consistent with the organization’s mission as expressed in this mission statement, develop a statement of philosophy for your department.
3. Write one major policy that supports this philosophy.
4. Write two or three specific procedures that express aspects of the policy from Question 3 as instructions for action (keeping in mind that a policy is ordinarily a statement of what is to be done, and a procedure consists of how it should be done).
EXERCISE: PLANS ARE WHAT?
Consider the following statement: plans in and of themselves are not especially useful; however, the planning process is invaluable.
In essay form, thoroughly explain what you believe is meant by this statement. It will be necessary to examine the statement from both directions. That is, explain the truth (or lack thereof) in the comment about plans not being especially useful, and then proceed to explain the supposedly greater value of the planning process.
EXERCISE: GOALS, OBJECTIVES, AND PROCEDURES
For any department of your choosing (except for physical therapy and health information management, which are used in this chapter’s examples), create a general objective that identifies the department’s overall mission, and provide a set of three to five functional objectives describing how the general objective will be pursued. Then select one of the functional objectives and in outline form create at least one procedure that could be applied in pursuing that objective.
CASE: PAID TO MAKE DECISIONS?
Background
Carrie Wilson, a registered nurse with more than 10 years of active supervisory experience, was hired from outside as nursing manager for the emergency department of County Hospital. It was Carrie’s style to develop insight into how to manage a given operation by putting herself where the action was and becoming totally immersed in the work. She quickly discovered, however, that her tendency to become deeply involved in hands-on work drew reactions from staff members ranging from surprise to resentment. She also discovered that her predecessor, who had been in the position for several years, had been referred to as the “Invisible Nurse.” As someone said about the former manager, “I think she was a very pleasant person, but that’s hard to say because we almost never saw her.”
In spite of the legacy of the Invisible Nurse, Carrie provided a constant management presence and seemed determined to remain deeply involved in the work of the department. She was also determined to vastly improve the level of professionalism in the department, a quality that had struck her from the first as decidedly lacking.
In a short time, Carrie had moved to reinstate and enforce a long-ignored dress code for the department, eliminate personal telephone calls during working hours except for urgent situations, curb chronic tardiness on the part of some staff members, bar food and drink and reading materials from work areas (also a reemphasis of long-ignored rules), and curb the practice of changing scheduled days of work after the time limit allowed by policy.
Carrie found her efforts frustrated at every turn. As she said to her immediate superior, “I can’t understand the reaction. All I’ve done is insist that a few hospital rules be followed—mostly rules that have been there all along but were being ignored—and added a few twists unique to the emergency department. Just that, and yet the bitterness and lack of support and even resentment are so strong I could slice them. I’m getting all-out resistance from a few people whom I would still have to describe as good, professional nurses at heart.”
Carrie’s boss, the vice president for nursing service, said, “Do you suppose you may have been pushing too hard, hitting them with one surprise after another without knowing how they felt and without asking for their cooperation?”
“That’s possible,” answered Carrie, “but now I’m committed on several fronts and I can’t back down on any of them without looking bad to the department.”
“Don’t think of this as a contest of wills or a game,” said the vice president. “It may be necessary for you to back down temporarily in some areas or at least hold a few of your improvements up in the air for a while. It may not hurt to fall back and involve a few of your staff in looking at the apparent needs of the department.”
With a touch of impatience in her voice, Carrie said, “Oh, I’ve heard all this stuff about participative management and staff involvement in making decisions. That may be the way for some, but that’s never been my style. I’m paid to make decisions so I make them—I don’t try to avoid responsibility by encouraging employees to make my decisions.”
Questions
1. What are the weaknesses, if any, in Carrie’s final statement about decision-making responsibility?
2. What has essentially been wrong with Carrie’s approach to raising the level of professionalism in the department?
3. How has Carrie’s behavior altered or otherwise affected the environment within which she expects her decisions to be implemented?
4. Ideally, how should Carrie have initially approached her plan to improve the emergency department?
5. Given the state of affairs Carrie is facing as of her conversation with the vice president, how should she go about attempting to salvage some of her ideas and proceed with the improvement of the department? Keep in mind that at this stage her actions have probably had serious effects on her chances of implementing her plans, and some of the decisions she may have already made may need to be revisited in a different fashion.
NOTES
1. Chester Barnard. The Functions of the Executive (Cambridge, MA: Harvard University Press, 1968), 202.
2. Charles Lindblom, “The Science of Muddling Through,” Public Administration Review (Spring 1959): 79–88.
3. Herbert Simon, Models of Man (New York: John Wiley & Sons, 1957), 207.
4. Vilfredo Pareto, Mind and Society (New York: Harcourt, Brace, 1935).
5. Grant Hammond. The Mind of War: John Boyd and American Security (Washington, DC: Smithsonian Institution Press, 2001).



