Public Health Homework
PAGES 235-237
Planned Approach to Community Health, Model Standards, and Community Health Improvement Processes In addition to the essential public health services framework and the APEXPH/MAPP processes, the IOM report stimulated several other important initiatives to promote core function-related performance, especially for the assessment and policy development functions. As described in Chapter 2, new national health objectives and a panel of leading health indicators were established for the year 2020, based on 3 decades of experience with the year 1990, 2000, and 2010 national health objectives. Broader participation in their design and more concerted strategies for their implementation in community settings distinguish the year 2020 objectives from the three earlier efforts. One of the first community health planning tools to be widely used was the Planned Approach to Community Health (PATCH), a process for community organization and community needs assessment that emphasizes community mobilization and constituency building. PATCH focuses on orienting and training community leaders and other community participants in all aspects of the community needs assessment process and includes excellent documentation and resource materials. Although originally developed by the Centers for Disease Control and Prevention (CDC) to focus on chronic health conditions and stimulate health promotion and disease prevention interventions, PATCH is flexible enough to be used in a wide variety of community health needs assessment applications.
Another important tool for addressing public health core functions and their associated processes is Model Standards, Healthy Communities.
The steps outlined for implementation of the Model Standards process in the community link many of the various core function-related tools; they represent, in effect, a pathway for organizations to participate in community health improvement activities.
1. Assessment of organizational role. Communities are organized and structured differently. As a result, the specific roles of local public health organizations will vary from community to community. An essential first step is to reexamine organizational purpose and mission and develop a long-range vision through strategic planning involving its internal and external constituencies. The resulting mission statement and long-range vision serve to guide the organization (leadership and board, as well as employees) and to define it for its community partners. This critical step should be completed before the remaining steps can be successfully addressed. Part I of APEXPH and the expanded strategic planning elements of MAPP are useful in accomplishing this task.
2. Assessment of organizational capacity. After mission and role have been defined, it is necessary to examine an organization’s capacity to carry out its role in the community. This calls for an assessment of the major operational elements of the organization, including its structure and performance for specific tasks. This type of organizational and local public health system self-assessment is best carried out through broad participation from all levels. Both APEXPH and MAPP include hundreds of indicators that can be used in this capacity assessment. These indicators can be modified or eliminated if deemed inappropriate, and additional indicators can also be used. This step serves to identify strengths and weaknesses relative to mission and role.
3. Development of a capacity-building plan. The development of a capacity-building plan incorporates the organization’s strengths and prioritizes its weaknesses so that the most important are addressed first. As in any plan, specific objectives for addressing these weaknesses are developed, responsibilities are assigned, and a process for tracking progress over time is established. Again, APEXPH and MAPP are valuable tools for accomplishing this task.
4. Assessment of community organizational structure. Having looked internally at its capacity and ability to exercise its leadership role for identifying and addressing priority health needs in the community, the public health organization must assess the key stakeholders and necessary participants for a community-wide needs assessment and intervention initiative. This is often a long-term and continuous process in which the relationship of all important community stakeholders and partners (e.g., the health agency, community providers of health-related services, community organizations, community leaders, interest groups, the media, and the general public) is assessed. This step determines how and under whose auspices community health planning will take place within the community. Both APEXPH/MAPP and PATCH processes support the successful completion of this step.
5. Organization of community. This step calls for organizing the community so that it represents a strong constituency for public health and will participate collaboratively in partnership with the health agency. Specific strategies and activities will vary from community to community but will generally include hearings, dialogues, discussion forums, meetings, and collaborative planning sessions. The specific roles and authority of community participants should be clarified so that the process is not perceived as one driven largely by the health agency and so-called experts. Both APEXPH/MAPP and PATCH are useful for completing this step.
6. Assessment of community health needs. The actual process of identifying health problems of importance to the community is one that must carefully balance information derived from data sets with information derived from the community’s perceptions of which problems are most important. Often, community readiness to mitigate specific problems greatly increases the chances for success, as well as support for the overall process within the community. In addition to generating information on possible health problems, this step gathers information on resources available within the community. This step serves to provide the information necessary for the community’s most important health problems to be identified. The community needs assessment tools provided in both APEXPH/MAPP and PATCH can be used to accomplish this step.
7. Determination of local priorities and community health resources. After important health problems are identified, decisions must be made as to which are most important for community action. This step requires broad participation from community participants in the process so that priorities will be viewed as community rather than agency-specific priorities. Debate and negotiation are essential for this step, and there are many approaches to coming to consensus around specific priorities. Both APEXPH/MAPP and PATCH support this step.
8. Selection of outcome objectives. After priorities are determined, the process must establish a target level to be achieved for each priority problem. For this step, the Model Standards process is especially useful in linking community priorities to national health objectives and establishing targets that are appropriate for the current status and improvement possible from a community intervention. This step also calls for negotiation within the community because deployment and reallocation of resources may be needed to achieve the target outcomes that are agreed upon. In addition to Model Standards, both APEXPH/MAPP and PATCH can be useful in accomplishing this step.
9. Development of intervention strategies. This step is one of determining strategies and methods of achieving the outcome objectives established for each priority health problem. This can be quite difficult and, at times, contentious. For some problems, there may be few or even no effective interventions. For others, there may be widely divergent strategies available, some of which may be deemed unacceptable or not feasible. After agreement is reached as to strategies and methods, responsibilities for implementing and evaluating interventions will be assigned. With community-wide interventions, overall coordination of efforts may also need to be addressed as part of the intervention strategy.
10. Implementation of intervention strategies. After the establishment of goals, objectives, strategies, and methods, specific plans of action for the intervention are developed, and specific tasks and work plans are developed. Clear delineation of responsibilities and time lines is essential for this step.
11. Continuous monitoring and evaluation of effort. The evaluation strategy for the intervention will track performance related to outcome objectives, as well as process objectives and activity measures over time. If activity measures and process objectives are being accomplished, there should be progress toward achieving the desired outcome objectives.
If this does not occur, the selected intervention strategy needs to be reconsidered and revised. Since 1990, numerous communities have used PATCH, Model Standards, and other tools (such as Healthy Cities and Healthy Communities, two similar community needs assessment processes) in community health-improvement initiatives. In 1996, and again in 2002, the IOM revisited issues addressed in The Future of Public Health report, concluding that different organizations, leadership, and political and economic realities were transforming how public health carried out its core functions and essential services.16,17 On one hand, market-driven health care was forcing public health to clarify and strengthen its public role in a predominately private system. On the other, public health was increasingly identifying and working with a variety of entities within the community that shape community health and well-being. Another important IOM report18 in 1997 advanced an expanded CHIP model that extends the tools developed earlier in the decade and the steps described previously here. Its main features are its expanded perspective on the wide variety of factors that influence health, its support for broad participation by community stakeholders, and its emphasis on the use of performance measures to ensure accountability of partners and track progress over time. Community health assessments leading toward community health improvement plans increased in quantity as well as quality during the two decades between 1990 and 2010. A survey conducted by NACCHO in 2008 found that nearly two thirds of local health jurisdictions (LHJs) nationwide had conducted a community health assessment in the past 3 years and nearly 70% planned to complete one within the next 3 years (Figure 5-3).19 Those not planning to conduct assessments were primarily the smallest LHJs with few full-time employees (Figure 5-4). Similar patterns were identified for community health improvement plans. The most widely used tools for assessment and planning are APEXPH/MAPP and state-specific tools. Metropolitan LHJs are more likely to develop their own assessment tools, whereas nonmetropolitan LHJs are somewhat more prone to use tools developed at the state level. The expanded use of these tools underscores the importance of community health improvement indicatives as a hallmark of 21st century community public health practice. As documented in Figure 5-5, LHDs play leadership or partnership roles in nearly all LHJs involved with community health planning.
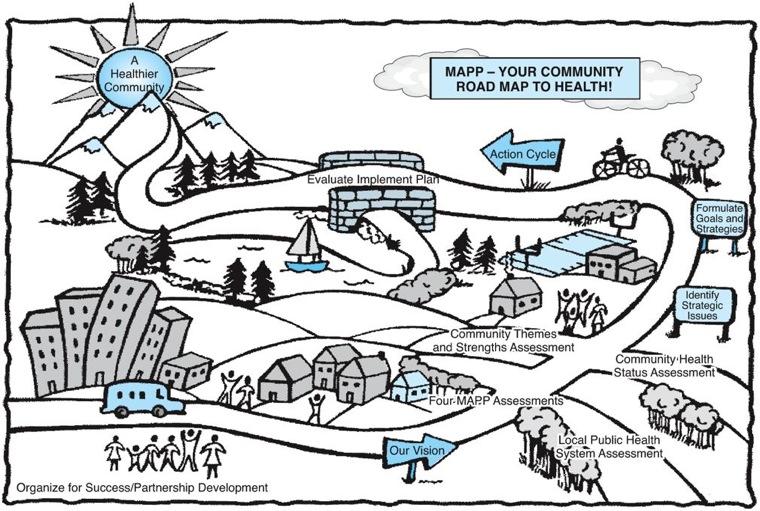
There is no fixed or even preferred sequencing of its components. The boundaries of the model identify the four assessments that comprise the MAPP process; these are usually completed after visioning has taken place but before strategic issues are identified in the steps indicated in the center of the model. Each element of the model is briefly described here:
• Organizing for success/partnership development—involves establishing values and outcomes for the process and determining the scope, form, and timing for planning process, as well as its participants.
• Visioning—involves developing a shared vision of the ideal future for the community, which serves to provide the process with focus, purpose, direction, and buy-in.
• Four MAPP assessments—these inform the planning process and drive the identification of strategic issues. All are critical to the success of the process, although there is no prescribed order in which they need to be undertaken. The four strategic assessments are as follows:
– Community themes and strengths
—involves the collection of inputs and insights from throughout the community in order to understand issues that residents feel are important.
– Local public health assessment
—involves an analysis of mission, vision, and goals through the use of performance measures for the essential public health services. Both strengths and areas for improvement are identified.
– Community health status assessment
—involves an extensive assessment of indicators in 11 domains, including asset mapping and quality of life; environmental health; socioeconomic, demographic, and behavioral risk factors; infectious diseases; sentinel events; social and mental health; maternal and child health; health resource availability; and health status indicators
– Forces of change
—identifies broader forces affecting the community, such as technology and legislation.
• Identify strategic issues—involves fundamental policy questions for achieving the shared vision, arising from the information developed in the previous phases. Some are more important than others and require action.
• Formulate goals and strategies—involves developing and examining options for addressing strategic issues, including questions of feasibility and barriers to implementation. Preferred strategies are selected.
• The action cycle—involves implementation, evaluation, and celebration of achievements after strategies are selected and agreed on.
As depicted in Figure 5-2, MAPP serves as a virtual road map for community public health systems. Widespread use of MAPP began in 2001, and after only a few years its impact was apparent in an evaluation of 130 early adopters.15 Figure 5-2 MAPP as a road map for community public health systems. Source: From National Association of County and City Health Officials, 2000.