HCA 415: Community and Public Health- Public Health Disasters & Preparedness
11.1 Introduction
For many people in the United States and around the world, September 11, 2001, began an era of terrorism. With the destruction of the New York City's World Trade Center towers and the Pentagon as well as the plight of Flight 93, Americans were no longer exempt from the terrorism that seemed more commonplace in other parts of the world (Yeboah, Chowdhury, Ilias, Singh, & Sparks, 2007).
Surprisingly, terrorism is not new to the United States and has occurred on American soil since the early 1800s. Some would argue that terrorism began as soon as Christopher Columbus discovered America and the "White man" battled with the Native Americans. Regardless of the point at which it began, it is not a new concept. What is relatively new is bioterrorism, which first began only in the mid-1980s (Resnick, 2013).
The September 11, 2001, attacks on the World Trade Center changed the way Americans viewed terrorism. Even though terrorist attacks were not new to the United States, September 11th proved a vivid example of how vulnerable the country could be in times of crisis.
This chapter will discuss the history of terrorism and bioterrorism and will explain the past and current responses of the United States to such incidents. It will also delve into the role of public health emergencies with a focus given to the principles of emergency response and preparedness and the agencies charged with coordinating efforts to keep our nation safe.
This chapter will also discuss the role of emergency response and preparedness of all types of disasters, both man-made and natural. Some elements we will discuss include disasters such as the Exxon Valdez oil spill; the Picher, Oklahoma, lead contamination; the Three Mile Island nuclear disaster; the Niagara Falls Love Canal; the Libby, Montana, asbestos contamination; and the Gulf oil spill (Institute of Medicine, 2006; Mother Nature Network, 2013).
This chapter will also touch upon natural disasters, including the 1871 Great Chicago Fire; the 1889 Johnstown, Pennsylvania, flood; the 1900 Galveston, Texas, hurricane; the 1906 Great San Francisco Fire and Earthquake; the 1930s Dust Bowl in the Great Plains; the 1988 heat wave in Plain states; the 1993 Storm of the Century blizzard; the 1999 F5 tornado in Oklahoma; and 2005's Hurricane Katrina (Frater, 2010; Nguyen, 2007).
Finally, we will discuss bioterrorism and various acts that have transpired over the last 50 years. This includes the 1970s toxic chemicals that were sent through the mail to government officials; the 1972 failed attempt at poisoning the Chicago water supply; the 1984 anthrax-tainted salad bars in Oregon; the 9/11 attacks and subsequent anthrax scares; and the 2013 ricin scares (Anti-Defamation League, 2005; Higgins et al., 2003; Klietmann & Ruoff, 2001; and Ward, 2013).
While this chapter describes these attacks and incidents, the concentration will be on the role of public health in coordinating responses, actions, relief, and clean-up efforts to maintain the health of the nation as well as the environment.
Defining Terrorism, Bioterrorism, Emergencies, and Response
Defined in Title 22 of the United States Code, Section 2656f(d), terrorism means an act of violence against innocent civilians or unarmed groups/individuals by national, secretive, or undercover groups (United States Code, 2004). The United States Code is a publication under the Office of the Law Revision Counsel of the United States that consolidates all of the laws of the nation into one document by subject heading (United States House of Representatives, n.d.).
Also in that code are definitions of international terrorism and terrorist group. The former means terrorism involving the citizens of more than one country; the latter is any group that practices international terrorism (United States Code, 2004).
Bioterrorism is slightly different from terrorism in that it encompasses the definition of terrorism, but involves the use of specific elements in carrying out the act. According to the Centers for Disease Control and Prevention (2013a), bioterrorism is terrorism using agents and organisms that pose a risk to human life, thus also posing a national security risk. A national security risk is outlined by four specific actions: (1) the agent used must be easily disseminated or transmitted by humans; (2) the result involves significant death rates, pointing toward a major public health impact; (3) the act causes public panic; and (4) the resulting incident requires public health preparedness and response in a specified manner (CDC, 2007). Bioterrorism contains three categories of agents, identified by the toxicity levels (we provide a complete list in Table 11.7):
Top priority actions are given to Category A agents, which include Bacillus Anthracis (anthrax), Clostridium botulinum (botulism), Yersinia Pestis (plague), and Variola (smallpox) (CDC, 2013n.d.). Released into a population, these agents constitute a national security risk because they fall under all four specified actions named above.
Category B agents are second in priority and are not nearly as deadly, although they can result in moderately increased disease acquisition among the human population. These include food safety threats such as Salmonella, E. coli, and Staphylococcal enterotoxin B; water safety threats such as cholera and cryptosporidium; and ricin (CDC, 2013n.d.).
Category C agents have been identified as any agent that could cause an emerging infectious disease such as a hantavirus, which has the potential for high deaths if it is readily available, produced, and disseminated (CDC, 2013n.d.).
What constitutes an emergency for one person may be a simple problem for another. The Federal Emergency Management Agency (FEMA) significantly distinguishes differences between the terms "hazards," "disasters," "emergencies," and other similar words (FEMA, 2008). In fact, it seemingly has yet to settle on an accepted definition, since the agency's training manual lists 18 individual definitions of the term "emergency" (FEMA, 2008). To pin down an exact definition may be impossible; however, in the context of national emergencies, the state of Rhode Island Department of Emergency Management (n.d.) has defined the word in the simplest of terms: An emergency is an incident that threatens public health, safety, and welfare.
States of emergency are quite different, as noted by FEMA, and are categorized as occurring locally, statewide, or nationally. Local emergencies are those that are confined to a geographical region of a state such as a city, county, or municipality. State of emergency is confined to one or more states within the nation. State of war emergency is just as the name implies: It is declared when anywhere in the nation is threatened or attacked by an enemy of the United States (FEMA, 2008).
Emergency preparedness encompasses all activities that are planned and implemented to manage an emergency (FEMA, 2008). These include not only the individuals and responsibilities of emergency response teams, but also the community's readiness to fulfill an emergency action plan.
Ford Theatre box seats in which President Abraham Lincoln was assassinated by John Wilkes Booth on April 14, 1865. Killings in protest of Lincoln's abolishment of slavery, including Lincoln's assassination, were among the very first acts of terrorism in the United States.
Emergency response is defined as the tactical planning and subsequent activities used to protect the public's health (environment and life). Included within this definition are evacuation plans, escalation protocols, damage reporting and assessment, medical team dispatch, salvage, search and rescue, and hazardous materials response and control (FEMA, 2008). Escalation protocols, which are necessary in an emergency, ensure that all emergency response personnel carry out their roles and responsibilities effectively and appropriately to protect the nation and promote the health and well-being of the American people. They are intended to prevent harm and reduce the risks of further danger and damages from the declared emergency.
In addition, FEMA (2013) defines several other terms that assist with the emergency planning and response process. A hazard is defined as something that is potentially dangerous and is likely the main cause for a disaster or emergency (FEMA, 2013). Threat is identified as an indication of possible harm or danger (FEMA, 2013). Threats can be naturally occurring such as a tornado or hurricane, man-made as in chemical explosions or industrial accidents, or intentionally human-caused such as terrorist acts.
History of Terrorism and Bioterrorism in the United States
While it may seem like a rare event on U.S. soil, terrorism (both domestic and international) has occurred in the country for centuries. News reports have indicated that major acts of terrorism have occurred as long ago as 1837 (Resnick, 2013).
While the present decade is experiencing terrorism through radical Muslim and al-Qaeda terrorist groups, the United States has seen other groups come and go over the past 2 centuries. These groups include the Ku Klux Klan, pro-slavery groups, Islamic extremists, Jewish extremists, leftist militants, Black militants, Puerto Rican nationalists, Palestinian militants, and many others.
See Figure 11.1 and Tables 11.1 and 11.2 for more details on when and where terrorism has occurred throughout the nation's past.
Figure 11.1: Number of confirmed acts of terror in the United States, 1800–2010
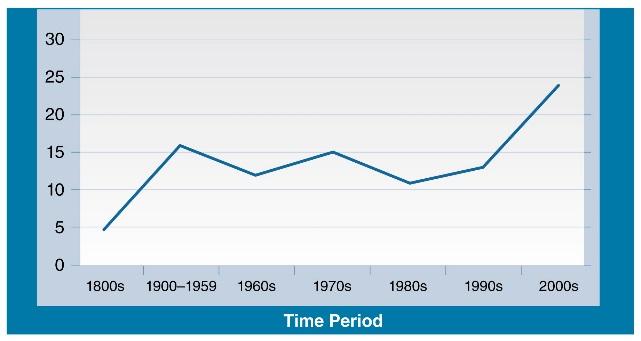
Source: Data from FBI. (2013). Retrieved from http://www.nctc.gov/site/index.html
| Table 11.1: Terrorism in the United States, 1800–present | ||
| Year(s) | Incident | Terrorist/Terrorist Group |
| 1837–1865 | Pro-Slavery Killings: Numerous killed throughout Kansas in opposition of President Abraham Lincoln's abolishment of slavery (Forums on Terrorism, Feminism, and Lincoln, 2002; Schaub, 2002). | Pro-slavery groups |
| 1865 | President Abraham Lincoln's Assassination: John Wilkes Booth, Lewis Powell, and George Atzerodt plot against the nation for abolishing slavery. President Lincoln is assassinated (Forums, 2002; Schaub, 2002). | Pro-slavery groups |
| 1910 | LA Times Bombing: Los Angeles Times building bombing by union supporters who were opposed to the newspaper's anti-union stance; 21 deaths (Irwin, 2013). | Pro-Union groups |
| 1915 | Harbor Island Explosion: Germans blow up a barge carrying 15 tons of gunpowder near the coast of Seattle, Washington, near Harbor Island. They were afraid the weapons would be used against them during World War I (Neiberg, 2013). | Anti-American group |
| 1916 | Preparedness Day Parade Bombing: Radical union leaders allegedly bomb San Francisco; 10 killed, 40 injured (Editorial Paragraphs, 1929). | Pro-Union groups |
| 1916 | Black Tom Explosion: Germans explode American ammunition supplies in Jersey City, New Jersey, in an attempt to prevent their use during World War I (Powles, 2004). | Anti-American groups |
| 1917 | Milwaukee Bombing: Anarchists were blamed for a bomb that exploded in Milwaukee; 9 officers and 1 civilian killed (Milwaukee's Finest, n.d.). | Anarchists |
| 1920 | New York City Bombing: TNT planted in an unattended horse-drawn wagon exploded on Wall Street; 35 died, hundreds injured (FBI, n.d.; "Wall Street Tragedy," 1993). | Bolshevist terrorists |
| 1921 | Tulsa Race Riot: Whites were blamed for released explosives from airplanes over Black ghettos in Tulsa; 300+ deaths, 1,100 homes destroyed (Messer, 2011). | White supremacists |
| 1927 | Bath School Disaster, Michigan: Bombs exploded the Bath Consolidated School; 45 killed (mostly children ages 7–12); 58 injured. This was considered the deadliest act of mass murder in a school at the time (Kim et al., 2010). | Unknown and unsolved |
| 1933 | Boeing 247 Explosion: This marks the first-ever terrorist attack through aviation; 7 killed (Arizona Wrecks, n.d.). | Unknown and unsolved |
| 1940 | New York City World's Fair: A bomb is exploded at the British Pavilion at the World's Fair; 2 injured policemen (Mauro, 2010). | Unknown and unsolved |
| 1940–1956 | The Mad Bomber: George Metesky placed more than 30 bombs throughout New York City in protest of high electricity rates; 10 injured (Delafuente, 2004; "The Mad Bomber," 1957). | Antigovernment; acting alone |
| 1958 | Hebrew Benevolent Congregation Bombing: The Temple is bombed in Atlanta, Georgia (Greene, 1996). | White supremacists |
| 1960 | The Sunday Bomber: A series of bombs explode in New York City subways; 1 death, 51 injured (Esposito & Gerstein, 2007). | Unknown and unsolved |
| 1969 | New York City Bombing: Radical leftist Jane Alpert bombs the United States Department of Commerce, Federal Building, Armed Forces Induction Center, and the Manhattan Criminal Court buildings ("Underground Odyssey," 1975). | Antigovernment (Black Panther movement) |
| 1970 | Stanford University Fires: Students set fires, break windows, and throw rocks into buildings on campus ("Tame Spring, Troubled Stanford," 1971). | Antigovernment student radical groups |
| 1974 | Alphabet Bomber: Muharem Kubegovich bombs the Pan Am terminal at the Los Angeles International Airport; 3 killed, 8 injured (Grad, 2008). | Antigovernment; Yugoslavian-born terrorist |
| 1975 | LaGuardia Airport Christmas Bomb: 11 killed, 75 injured ("The LaGuardia Blast," 1976). | Unknown and unresolved |
| 1975 | New York City Bombing: Historic Fraunces Tavern bombed; 4 killed, 50+ injured (United States Department of State, n.d.). | Puerto Rican militants |
| 1978–1995 | The Unabomber: 16 bombs sent through the mail by Ted Kaczynski; 3 killed, 23 injured (Zuk & Zuk, 2000). | Antitechnology |
| 1980 | Statue of Liberty Bombing: Bomb explodes in the statue's story room causing $18,000 in damages; no deaths or injuries (Kushner, 2003). | Croatian terrorists |
| 1993 | First World Trade Center Bombing: A bomb explodes in the underground parking garage of the World Trade Center, Tower 1; 6 killed, 1,042 injured (FBI, n.d.; "Wall Street Tragedy", 1993). | Al-Qaeda terrorists |
| 1995 | Oklahoma City Bombing: Timothy McVeigh sets off a car bomb that collapses most of the federal office building and damages more than 220 surrounding buildings; 168 deaths (Corley, Mlaker, Sozen, & Thornton, 1998; Fernandez, 2007). | Branch Davidian terrorist group |
| 1996 | Centennial Olympic Park Bombing: Eric Robert Rudolph plants pipe bombs underneath benches in Olympic Park during the 1996 Summer Olympics; 2 killed, 111 injured (FBI, n.d.). | Unknown terrorist group |
| 1997 | Empire State Building Shootings: A Palestinian opens fire on tourists on an observation deck; 1 killed; many injured (Johnson, 2007). | Palestinian terrorists |
| 2001 | 9/11: Airplanes flew into the World Trade Center towers and the Pentagon. Flight 93 was set to hit the White House but was brought down by the teamwork of the passengers. More than 2,700 people were killed; thousands more injured (Hess & Stoddard, 2011). | Al-Qaeda terrorists |
| 2001 | The Shoe Bomber: Richard Reid of Great Britain attempted to blow up a plane with a bomb in his shoe. Passengers thwarted his plan. No injuries (McDonald, 2011). | Al-Qaeda terrorists |
| 2002 | The Beltway Sniper: Two radical Muslim terrorists shoot at people on the Washington, D.C., beltway over the course of 3 weeks; 10 killed, 3 injured (Brumberg, 2003; FBI, n.d.; Lang, 2004). | Radical Muslim terrorists/Anti-American |
| 2006 | University of North Carolina SUV Attack: Radical Muslim Mohammed Reza Taheri-azar intentionally crashed his SUV into people. No deaths (Bandes, 2006). | Radical Muslim terrorists/Anti-American |
| 2009 | New York City Subway Bombing: An Afghan immigrant plots to bomb the New York City subway system. His plan was thwarted | Al-Qaeda terrorists |
| 2009 | Fort Hood Shooting: A Muslim psychiatrist opened fire on an Army base in Fort Hood, Texas; 13 deaths, 30 injured (Blumenfeld, 2013). | Muslim terrorists/Anti-American |
| 2009 | Little Rock Recruiting Office Shooting: Drive-by shooting at the office; 1 killed (Dao, Johnston, Barnes, & Delaqueriere, 2009). | Muslim terrorists/Anti-American |
| 2009 | Underwear Bombing Attempt: An attempt was made to blow up an airplane heading to Detroit, Michigan, with a bomb sewn into a man's underwear. Plot thwarted (Spencer, 2011). | Al-Qaeda terrorists |
| 2010 | Times Square Bombing Attempt: Pakistan native Faisal Shahzad plots to blow up Times Square with explosives in his car (Chuang & Roemer, 2013). | Pakistan militants |
| 2011 | Spokane Washington Bomb: A pipe bomb is discovered along the route of the Martin Luther King, Jr., Memorial March. No injuries (Richey, 2011). | Unknown and unsolved |
| 2013 | Boston Marathon Bombing. Two Chechnya natives explode bombs near the finish line of the Boston Marathon; 3 deaths, hundreds injured (CNN, 2013; Eligon et al., 2013). | Unknown at time of publication |
| Table 11.2: Bioterrorism in the United States | ||
| Year(s) | Incident: | Terrorist/Terrorist Group |
| 1970s | Alphabet Bomber & Chemical Warfare: Muharem Kurbegovic sends toxic chemicals through the mail to a Supreme Court justice and threatens to use nerve gas at the Capitol and against the president. This is before the bombing in 1974 (Anti-Defamation League, 2005). | Antigovernment; Yugoslavian-born terrorist |
| 1972 | Chicago Water Supply Thwarted Attack: Two college students, Allen Schwander and Stephen Pera, plan to poison the city's water supply with typhoid and other bacteria (Anti-Defamation League, 2005). | R.I.S.E. (acronym undefined) |
| 1984 | Rajneeshee Bioterror Attack: The Rajneeshee movement infect salad bars with Salmonella in 10 Dalles, Oregon, restaurants; 751 people were sickened, 40 hospitalized (Klietmann & Ruoff, 2001). | Rajneeshee terrorist group |
| 2001 | Anthrax Attacks: Infected letters are mailed to media and congressional offices by biologist Bruce Ivins, who was attempting to bring attention to his anthrax vaccine program (Higgins et al., 2003). | No group affiliation |
| 2013 | Ricin Attacks: Actress Shannon Guess Richardson sent letters laced with ricin to President Barack Obama, Senator Roger Wicker (R-Miss.), and a judge in Lee County, Mississippi (Ward, 2013). Richardson had intended to implicate her estranged husband, with whom she was embattled in divorce proceedings, in the crime. | No group affiliation |
11.2 Federal, State, and Local Agencies
Although terrorism has existed since the 1800s, the United States's vulnerabilities were tested to its limit in 2001 with the events of 9/11 and subsequent anthrax attacks. Since that time, the nation has evolved significantly with its protocols for preparing and handling emergencies. In the event of a national emergency—whether terrorist attack, bioterrorism threat, or disaster—there are certain protocols that apply in accordance with the Homeland Security Act of 2002. Numerous governmental agencies take action immediately in the event of an emergency within the country's borders. Of course, the Department of Homeland Security takes the lead, but it then guides upwards of 23 federal agencies that are involved with coordinating efforts during a national emergency.
The Department of Homeland Security (DHS)

© Martin H. Simon/Corbis
President George W. Bush signed legislation creating the Department of Homeland Security on November 25, 2002, as a means to protect the United States from foreign and domestic terrorism following the September 11th attacks. Upon its creation, the new department hired roughly 170,000 employees.
In response to the terrorist attacks on September 11, 2001, the Department of Homeland Security was created to provide stronger protections from domestic and international terrorism. Its primary mission is to protect the American homeland (Koenig, 2003). From a public health perspective, this means improved emergency preparedness and cooperation with all levels of government. The American Public Health Association assisted in developing the roles and responsibilities for this new department, developed and passed under the Bush Administration in 2002 (Late, 2002).
As mentioned earlier, the DHS comprises 23 different federal agencies, all of which play a key role in the health and safety of the nation's population. Three former United States Health and Human Services emergency response programs now operate under the DHS: the National Disaster Medical System, which coordinates and dispatches medical teams to disaster locations; the National Pharmaceutical Stockpile, which handles drugs and medical supplies for use during disasters; and the Metropolitan Medical Response System, which develops or enhances emergency preparedness in dealing with "weapons of mass destruction" (e.g., bioterrorism) (Late, 2002, p. 5).
The largest entity included under the DHS is the Federal Emergency Management Agency (FEMA), which responds under the Robert T. Stafford Disaster Relief and Emergency Assistance Act (P.L. 93-288). This act, which went into effect in the fall of 1988, contains significant responsibilities for preparedness and response in the event of any emergency. Refer to Health Care in Action: The Robert T. Stafford Disaster Relief and Emergency Act for more details on this act.
Health Care in Action: The Robert T. Stafford Disaster Relief and Emergency Act

Time & Life Pictures/Getty Images
Then-Senator Richard Nixon shown here putting out brush fires on the roof of his Los Angeles home on November 1, 1961. As president, Nixon went on to sign the Disaster Relief Act of 1970, which was intended to provide funding to those affected by natural disasters.
Signed into law on November 23, 1988, this act amended the 1974 Disaster Relief Act. Of interest is the fact that the 1974 act in turn had amended the Disaster Relief Act of 1970 to further extend assistance from the federal government to states, local communities, and individuals in the event of a disaster such as a tornado (Peters, 2013). The Disaster Relief Act of 1970 was the first federal disaster relief law in the United States. President Richard Nixon found that the increasing number of major disasters, mostly natural disasters, were financially hurting businesses, organizations, individuals, and communities across the nation. This original act (of 1970) provided financial relief to help rebuild. It included four key items: (1) a property tax revenue maintenance plan for those whose tax bases were destroyed through the disaster; (2) the authority to repair or replace damages to public buildings; (3) improvements to the loan programs that assist people in the event of loss from the disaster; and (4) authority for the federal government to assist with lessening the effects of the disaster.
The most recently amended act, now known as the Robert T. Stafford Disaster Relief and Emergency Act, encompasses far more than natural disasters. The law states:
It is the intent of Congress, by the Act, to provide an orderly and continuing means of assistance by the Federal Government to State and local governments in carrying out their responsibilities to alleviate the suffering and damage which result from such disasters by:
Revising and broadening the scope of existing disaster relief programs;
Encouraging the development of comprehensive disaster preparedness and assistance plans, programs, capabilities, and organizations by the States and by local governments;
Achieving greater coordination and responsiveness of disaster preparedness and relief programs;
Encouraging individuals, States, and local governments to protect themselves by obtaining insurance coverage to supplement or replace governmental assistance;
Encouraging hazard mitigation measures to reduce losses from disasters, including development of land use and construction regulations; and
Provide Federal assistance programs for both public and private losses sustained in disasters.
Source: FEMA (2007, p. 13).
Since the Stafford Act passed, numerous amendments were made as a result of the 2004 Hurricane Katrina disaster. This affected several sections of the act, including firearms policies, detailed administrative functions, and community disaster loans. Also as a result of the amendments, two additional acts were passed: The Pet Evacuation and Transportation Standards Act of 2006 and the Security and Accountability for Every Port Act of 2006 (FEMA, 2007). The former addresses the needs of pet owners and those with service animals (GovTrack, 2006), and the latter addresses safety and security needs at all United States Maritime Facilities (United States Government Printing Office, 2006).
Federal Emergency Management Agency (FEMA)
FEMA's mission is "to support our citizens and first responders to ensure that as a nation we work together to build, sustain, and improve our capacity to prepare for, protect against, respond to, recover from, and mitigate all hazards" (FEMA, 2013, para. 4).

© Bowden/AP/Corbis to Bowden/Associated Press
In March 1979, the Three Mile Island nuclear power plant leaked radioactive gas from one of the plant's reactors inciting President Carter to bring together the varied disaster relief agencies under FEMA.
FEMA has a long history, having started under no particular organizational name through the Congressional Act of 1802, which is considered the nation's first piece of disaster legislation. At that time, the act was passed so that funds could be released to assist a New Hampshire community recovery from a devastating fire. Growing disaster relief demands from across the nation eventually prompted the development of the Reconstruction Finance Corporation in the 1930s (FEMA, 2013). Its main responsibility was to provide disaster loans to cities to repair or rebuild public buildings following disasters, mainly of the natural kind. Unfortunately, disaster relief was very fragmented as various earthquakes, floods, and hurricanes forced other agencies into action, including the Federal Disaster Assistance Administration (part of the Department of Housing and Urban Development), as well as federal and state entities connected with the National Flood Insurance Act, and the 1974 Disaster Relief Act. According to FEMA (2013), more than 100 federal agencies were involved when disasters and emergencies hit the nation, making relief efforts difficult to manage.
It wasn't until 1979, following the Three Mile Island Nuclear Meltdown disaster, when President Jimmy Carter ordered disaster relief agencies to work under one central command: the Federal Emergency Management Agency. Ever since FEMA was born, disasters have morphed beyond the natural kind and into man-made emergencies, such as the Exxon Valdez oil spill and terrorist attacks such as the September 11, 2001, attacks and the 2013 Boston Marathon bombing.
FEMA's main role is to coordinate efforts of preparedness, response, and recovery. The components of FEMA include the Office of Response and Recovery, Federal Insurance and Mitigation Administration, Mission Support Bureau, Protection and National Preparedness, and the United States Fire Administration. Depending upon the nature of the disaster, FEMA dispatches the protocol designed to handle the emergency. We will cover more on FEMA's actual responsibilities later in this chapter.
Other Federal Public Health Agencies
Monitoring Health in the United States and Beyond
The history and mission of the Centers for Disease Control.
Critical Thinking Question:
Explain how a small, localized community health campaign became the CDC. Can you think of any other major programs or sub-agencies that started out in a similar way?
Many other independent agencies also play a role in emergency preparedness and response. These include the Centers for Disease Control and Prevention, the Office of Public Health Emergency Preparedness and Response (OPHEP), the Health Resources and Services Administration (HRSA), the Food and Drug Administration (FDA), the National Institutes of Health (NIH), and the Federal Bureau of Investigation (FBI).
Centers for Disease Control and Prevention (CDC)
The Centers for Disease Control and Prevention (CDC) works with FEMA to assist with various disasters, which are categorized as natural/weather disasters, bioterrorism, chemical emergencies, outbreaks/incidents, mass casualties (explosions), and radiation emergencies (CDC, 2001a). While its website is the primary public source for information on emergencies (both in terms of personal response and preparedness), the organization does far more in disaster situations. The CDC has two primary functions in the event of an emergency: public health preparedness and medical preparedness. The former helps our nation (individuals, community, and the nation as a whole) protect against health emergencies. The latter works with the health care system to ensure it is prepared to handle and recover from a health emergency.
Office of Public Health Preparedness and Response (OPHPR)
Under the auspices of the CDC, the Office of Public Health Preparedness and Response (OPHPR) provides the strategic direction and coordination of efforts to prepare and respond to a crisis. An example of the CDC's responsiveness to public health emergencies is their annual preparations for seasonal influenza. The organization is charged with ensuring that the flu vaccine is not only available, but that it is also effective for the coming season. For the 2012–2013 season, the vaccine was widely available, and thus, the CDC did an exceptional job with maintaining a solid supply of seasonal influenza vaccine (CDC, 2013b). To continue to monitor the effectiveness throughout the entire season, the CDC has a monitoring system known as the United States Influenza Vaccine Effectiveness Network (CDC, 2013a). This tracks cases of all influenza strains so that it can focus its efforts by region of highest incidence. The network is a partnership between the CDC and many state and territorial health departments, along with various health-related entities (laboratories, clinics, and vital statistics offices) to monitor incidences of influenza. According to the CDC (2012), surveillance information is collected in five categories: incidence numbers; tracking influenza-related illnesses; determining which viruses are currently circulating; detecting any changes in the virus itself; and measuring the impact on hospitalizations and deaths across the nation.

AFP/Getty Images
In West Trenton, New Jersey, members of a hazmat team decontaminate an investigator of the anthrax attacks of 2001. Such investigators are part of the CDC's effort to mitigate the spread of disease.
Response to the anthrax scares of 2001 prompted the CDC and OPHPR to develop a training course on the communications efforts needed during a bioterrorism attack. The CDC's role in such efforts focused on cooperation with all emergency response teams, as well as minimizing widespread panic (Courtney, Cole, & Reynolds, 2003). During the actual crisis itself, the CDC provided field investigators to determine the spread of the disease, as well as the potential for stopping its progress in those already infected. The concept was to lessen the impact by confining the infected as much as possible. A central command center provided the link between the field agents and other emergency responders, as well as to the community at large. In addition, the CDC provided the potentially exposed with a 60-day course of antibiotics to combat further spread of the deadly weapon both domestically and abroad (Malecki et al., 2001). According to Polyak et al. (2002), the CDC's epidemiologists, laboratory scientists, and clinicians were asked to assist with anthrax inquiries around the world: 130 requests from 70 countries and 2 territories. The results helped alleviate worldwide panic, prevent unnecessary antibiotic treatment, and enhance international surveillance of bioterrorism events (Polyak et al., 2002).
Health Resources and Services Administration (HRSA)
The Health Resources and Services Administration's (HRSA) main function in the event of a disaster is to disseminate grants to presidentially declared disaster areas. Only through FEMA can HRSA provide financial assistance (HRSA, 2012). According the HRSA guidelines set by FEMA, the disaster funds can only be used after local emergency management assistance cannot handle the expenditure alone (HRSA, 2012). The following steps must be followed in order to acquire disaster funding from HSRA.
Major disaster declaration steps:
Local government responds first. If overwhelmed, it must seek state funds first.
The state responds with resources such as the National Guard or other financial resources.
Damage assessment is performed through local, state, federal, and volunteer agencies to determine losses and recovery needs.
A Major Disaster Declaration is requested by the state's governor, with state funds allocated to recovery.
FEMA evaluates the request and recommends action from the White House.
The president approves or denies the request, a process that could take a few hours or weeks, depending on the scope of the disaster.
Food and Drug Administration (FDA)
The United States Food and Drug Administration (FDA) oversees the development of human and veterinary products, as well as monitoring the food and blood supplies for the United States (FDA, 2012). Operating under FDA, the Office of Counterterrorism and Emerging Threats (OCET) facilitates the development of safe and effective medical countermeasures in the event of a terrorist or bioterrorist attack (FDA, 2012). As part of its duties, the OCET is charged with coordinating emergency use activities, as well as communication efforts within and outside the agency. Among the OCET's many counterterrorism programs are the following (FDA, 2012):
Animal and Veterinary Products and Counterterrorism—This program monitors animal foods and veterinary drugs for safety, as well as various other food and drug concerns. In the event of an emergency, this agency has numerous responsibilities to ensure safe food and drugs for the nation. Two of these responsibilities include the prevention of further distribution of contaminated feed and timely approval of animal drugs in the event primary facilities are overtaken or lost.
Biologic Product Security—This program focuses on the safekeeping of stockpiles of biological products such as medical supplies, bacterial and viral vaccines, and blood. It also works to expedite the development and licensing of products that will diagnose, treat, or prevent diseases following an exposure to bioterrorism agents.
Drug Preparedness and Bioterrorism—The program focuses solely on making sure there are adequate supplies of medicines and vaccines to protect the American public in the event of a bioterrorism attack.
Food Defense—This program works with many agencies across the nation to protect the food supply by reducing the risk of tampering with the food and cosmetic supplies in the United States.
Medical Devices (Emergency Situations)—This program ensures that appropriate medical devices are available in the event of an emergency, such as diagnostic equipment and tests, surgical tools, and personal protective equipment. While this is applicable to all emergencies, it was intended to focus on natural phenomenon like extreme weather (floods, hurricanes, tornadoes, and earthquakes).
National Institutes of Health (NIH)
The National Institutes of Health (NIH) comprises 27 institutes and centers, each focused on a different aspect of health research (National Institutes of Health, 2013). Each agency has its own focal point in the event of a disaster that is beyond the scope of this textbook; however, there is one particular program that has been especially helpful during acts of terrorism. The NIH's Institute of Neurological Disorders and Stroke (NINDS) operates a program known as NIH CounterACT (NINDS, 2013). This program focuses on developing new and improved medical countermeasures that will prevent, diagnose, and treat conditions caused by chemical threats (NINDS, 2013). For example, substances that could be used as biological weapons include arsenic trioxide, hydrogen sulfide, cyanide, tetramine, bromine, and ammonia (NINDS, 2013). The NIH supports efforts to find treatments and prevention vaccinations of the effects of exposure to such substances.
Federal Bureau of Investigation (FBI)
The Federal Bureau of Investigation (FBI) is the federal agency that we might as well consider the front line personnel in all terroristic acts. Its employees are the ones who investigate acts and potential acts of terror. The Bureau comprises multiple operations, including Joint Terrorism Task Forces, the Terrorist Screening Center, the Genocide and War Crimes Program, and Weapons of Mass Destruction (FBI, n.d.). It also operates numerous training programs, including the Hazardous Devices School, Resources for Law Enforcement, K-9 Bomb Detection, and Improvised Explosives (FBI, n.d.).
While working with the aforementioned agencies among many others, the FBI provides protection for the nation's borders and seaports, colleges and universities, food supply, and human rights and freedoms (FBI, n.d.). Through field offices scattered throughout the country, the FBI's main function is to protect, investigate, and help dismantle extremist networks worldwide (FBI, n.d.). The FBI has an interesting counterterrorism site detailing the world's most dangerous groups and timelines, as well as an interactive timeline and map at http://www.nctc.gov/site/index.html.
State and Local Agencies
Homeland security and emergency services are available in every state and the District of Columbia (United States Department of Homeland Security, n.d.). Most of them are set up to work closely with state governments, state health departments, law enforcement, and other public health and safety organizations. Each state has its own set of unique emergencies. For example, the Plains states deal with drought, the East Coast states often suffer from hurricanes, the mountain states experience snowstorms and avalanches, and the West Coast states often encounter earthquakes.
Regardless of the type of emergency or the state in which it occurs, the local government entities are typically the ones who trigger the emergency response. Local law enforcement and fire departments are often the first dispatched groups. If the event is too difficult or overwhelming for local entities to contain, these groups connect with their state officials.
At whatever level of response, the mission of homeland security and emergency response is to lead, coordinate, and support public health and safety. Now, we will move onto describing the various types of emergencies to which these entities respond.
11.3 Types of Emergencies
Both FEMA and the CDC identify various types of emergencies, all of which require a plethora of agency involvement and assistance from local and state to federal. Here are the main events identified as types of emergencies by the CDC and FEMA. Table 11.3 shows a chronological list of some of the major natural disasters that have occurred within the United States, and Table 11.4 displays the man-made disasters.
| Table 11.3: Major natural disasters in the United States | |||
| Year | Type | Location | Fatalities; Damages |
| 1816 | Famine | United States | Unknown (Oppenheimer, 2003) |
| 1888 | Blizzard | East Coast | 400 deaths; $20 million (Pearson Education, 2012) |
| 1896 | Tornado | St. Louis, Missouri | 255–400 deaths; $2.9 billion (The Tornado Project, 2013) |
| 1900 | Hurricane | Galveston, Texas | 6,000–12,000 deaths; unknown costs (National Oceanic and Atmospheric Administration, 2000) |
| 1906 | Earthquake | San Francisco, California | 3,000–6,000 deaths; unknown costs (Davies, 2012) |
| 1925 | Tornado | Missouri, Illinois, Indiana, Kentucky, and Tennessee | 695 deaths; $1.65 billion (National Weather Service Weather Forecast Office, 2010) |
| 1927 | Flood | Arkansas, Illinois, Kentucky, Louisiana, Mississippi, and Tennessee | 250 deaths; $400 million (Encyclopedia Britannica, 2013) |
| 1928 | Hurricane | Leeward Islands, Puerto Rico, Bahamas, and Florida | 3,000 deaths; $800 million (Barnes, 1998) |
| 1936 | Flood | Pittsburgh, Pennsylvania | 45 deaths; $3 billion (Carnegie Library of Pittsburgh, 2013) |
| 1937 | Flood | Ohio, Kentucky, Indiana, and Illinois | 385 deaths; $5 billion (National Weather Service Weather Forecast Office, 2012) |
| 1950 | Blizzard | Eastern United States | 383 deaths; $70 million (Pearson Education, 2012) |
| 1960 | Tsunami | Hawaii and Alaska | 61 deaths; $500,000 (Igarashi, Kong, Yamamoto, & McCreery, 2011) |
| 1970 | Tornado | Lubbock, Texas | 26 deaths; $1.4 billion (National Weather Service Weather Forecast Office, 2013) |
| 1974 | Tornado | Illinois, Indiana, Michigan, Ohio, Kentucky, Tennessee, Alabama, Mississippi, Georgia, North Carolina, Virginia, West Virginia, and New York | 330 deaths, 5,484 injuries, unknown damages (National Oceanic and Atmospheric Administration, n.d.) |
| 1989 | Hurricane | Eastern North America | 86 deaths; $9 billion (Pearson Education, 2013) |
| 1992 | Hurricane | Florida and Louisiana | 61 deaths; $27 billion (Pearson Education, 2013) |
| 1993 | Blizzard | East Coast of North and Central America | 270 deaths; $6 billion (Pearson Education, 2013) |
| 1998–1999 | Landslide | Kelso, Washington | 0 deaths; $70 million (FEMA, 1998) |
| 2004 | Hurricane | Florida, Texas, and East Coast | 183 deaths; $43 billion (Pearson Education, 2013) |
| 2005 | Hurricane | Louisiana | 120 deaths; $10 billion (Pearson Education, 2013) |
| 2005 | Hurricane | Louisiana, Florida, Mississippi, and Alabama | 1,732 deaths; $100 billion (Nicosia, 2009; National Oceanic and Atmospheric Administration, 2005) |
| 2007 | Fire | California | 14 deaths; unknown damages (Lemonick, 2007) |
| 2011 | Tornado | Joplin, Missouri | 161 deaths; $3 billion (City of Joplin, 2011) |
| 2012 | Hurricane | Eastern United States | 140+ deaths; $75 billion (Porter, 2013) |
| Table 11.4: Major man-made disasters in the United States | |||
| Year | Type | Location | Fatalities; Damages |
| 1889 | Flood | Johnstown, Pennsylvania | 2,209 deaths; $17 million in damages ($425 in 2012 dollars) (Wharton-Michael, 2012) |
| 1919 | Asbestos contamina-tion | Libby, Montana | 200 deaths, 1,000+ sickened; unknown damage estimate. (Mother Nature Network, 2013) |
| 1931–1939 | Drought | Great Plains | Unknown (Hoerling et al., 2012) |
| 1948 | Smog | Donora, Pennsylvania | 20 deaths, 7,000 sickened; unknown damage estimates (Pennsylvania Department of Environmental Protection, 2013) |
| 1967 | Lead contamina-tion | Picher, Oklahoma | Unknown illnesses; $20 million in cleanup costs (Sillery, 2001) |
| 1978 | Toxic waste exposure | Niagara Falls, New York | (Note: Love Canal—see Case Study: Love Canal: The First Federal Disaster Area From Man-made Causes for details.) (Binns, 2004) |
| 1979 | Nuclear meltdown | Dauphin County, Pennsylvania | 0 deaths; unknown (Smithsonian, n.d.). |
| 1989 | Oil spill | Alaskan coast | 250,000 seabirds, 2,800 sea otters, 300 harbor seals, 250 bald eagles, 22 killer whales, and billions of salmon and herring eggs perished. (Mother Nature Network, 2013) |
| 2007 | Fire | California | 14 deaths; unknown damages (Lemonick, 2007) |
| 2007 | Structure collapse | Huntington, Utah | 0 deaths; unknown damages (Lemonick, 2007) |
| 2008 | Coal ash spill | Kingston, Tennessee | Unknown illnesses and damages (Mother Nature Network, 2013) |
| 2010 | Oil spill | Gulf of Mexico | 11 deaths and more than 400 species of birds and sea life were severely threatened. (Mother Nature Network, 2013) |
| 2013 | Fire | Colorado | 2 deaths; unknown damages; fire fighting expenses cost more than $5.5 million. (Gorski, 2013; Gurman & Robles, 2013) |
Technological, Man-Made Hazards, and Chemical/Radiation Emergencies
FEMA (2008) identifies nuclear waste disposal spills, toxic substances, hazardous materials accidents, utility failures, pollution, epidemics, explosions, and fires under this category. Among its lengthy list of chemical/radiation hazards, the CDC (2013b) lists poisons from plants or animals, blood agents, lung/pulmonary agents, poisonous metals, nerve gasses, toxic alcohols, solvents, and radiation exposure. Examples of this include the Three Mile Island nuclear meltdown on March 28, 1979 (Smithsonian, n.d.). This was considered America's worst nuclear power plant accident, where radioactivity leaked from one of the reactors into the surrounding community near Harrisburg, Pennsylvania (Smithsonian, n.d.).
There have been numerous disasters in the United States that emerged because of either natural or man-made causes. The first federal declaration of a disaster from a man-made cause came out of New York State in the neighborhood of Love Canal in Niagara Falls (Binns, 2004). It took nearly 26 years to fully clean up after toxic waste infiltrated the area starting in the 1920s. See Case Study: Love Canal: The First Federal Disaster Area from Manmade Causes for more details.
Case Study: Love Canal: The First Federal Disaster Area From Man-made Causes
This incident, which occurred over the course of 50 years, was one of the most significant industrial waste dumping incidents in the nation. In the 1920s, a man named William T. Love attempted to build a canal in a neighborhood in Niagara Falls, New York (the neighborhood was eventually renamed Love Canal). When the plans failed, the large canal area became a dumping ground for various garbage, including some toxic waste. In the 1940s, Hooker Chemical Company started emptying its industrial waste products into the canal and covering it with dirt. It was estimated that more than 80 different toxins were dumped into the canal.
In 1953, Hooker Chemical eventually sold that land to the local school district (with a price tag of only $1) for the construction of a new school. Two years later, a 25-foot area surrounding the school disintegrated, exposing the various toxic chemical drums left by Hooker Chemical. These drums had apparently filled with rainwater, in which the children played. Furthermore, when the city began constructing new sewer lines for low-income housing, sections of the abandoned canal broke, releasing more toxic waste into the system.
According to one report, "Love Canal residents reported exploding rocks, strange odors, and blue goo that bubbled up into basements" (Mother Nature Network, 2013, para. 3). However, the most immediate concern was the increase in asthma, miscarriages, mental disabilities, and numerous other health problems that plagued the residents of Love Canal; 56% of children born between 1974 and 1978 suffered from birth defects that were directly connected to the toxins from Love Canal.
This was the first time in the nation's history that an area was declared a federal disaster area from man-made causes.
In 1995, cleanup efforts were complete, and the neighborhood was taken off the National Priorities List by the Environmental Protection Agency.
Source: Binns (2004); Mother Nature Network (2013); Popkin (1986).
Natural Disasters and Severe Weather

Stock Connection/SuperStock
Iowa has experienced an unprecedented number of natural disasters in recent history. Repeated severe weather and flooding events encouraged the development of the Iowa Department of Public Defense, which mirrors FEMA's efforts at the state and local levels.
Both the CDC (2013b) and FEMA (2008) identify earthquakes, floods, hurricanes, tornadoes, tsunamis, blizzards, drought, volcanoes, mudslides, and extreme heat under this category. The worst earthquake in the history of the United States took place on March 27, 1964, in Prince William Sound, Alaska (United States Geological Survey [USGS], 2012). According to the USGS, the earthquake with a magnitude of 9.2, and its associated tsunami took 128 lives and caused more than $311 million in damage. Communities affected by the earthquake included Anchorage, Portage, Kenai, Kodiak, and Wasilla (USGS, 2012). The quake was felt throughout most of Alaska, as well as parts of Canada.
In terms of natural disasters, one of the worst states in the nation for sustaining the highest number of severe weather incidents is Iowa. See Case Study: Iowa: A Magnet for Natural Disasters for details.
Case Study: Iowa: A Magnet for Natural Disasters
Since 1990, Iowa has experienced 30 presidentially declared disasters, most of which revolve around severe weather (Iowa Homeland Security, n.d.a). From 1950 to 1969, Iowa experienced 10 flooding emergency declarations; from the 1970s through 1980s, another 10 declarations were made for flooding and severe storms; the 1990s brought 11 severe weather emergency declarations; and from 2000 to 2011, the state has had 17 presidential declarations of severe weather emergencies (Iowa Homeland Security, n.d.a).
Iowa's Emergency Management practices began in 1965 as the State Civil Defense Agency (Iowa Homeland Security, n.d.b). This organization coordinated emergency response and recovery efforts for disasters such as floods and storms. The 2009 Code of Iowa, Chapter 29C, clearly outlines the responsibilities for Iowa's emergency management team, now known as the Iowa Homeland Security and Emergency Management Division (HSEMD) under the Iowa Department of Public Defense (Iowa Homeland Security, n.d.a). Much like FEMA at the federal level, Iowa's HSEMD operates in the same manner, but only within the boundaries of Iowa. It supports local entities as they plan for and respond to emergencies. The division also provides training, technical assistance, communications, and other emergency preparedness and response for municipalities within Iowa's 99 counties.
HSEMD is the coordinating body for all emergencies within Iowa. See Figure 11.2 for an illustration of its organizational structure and support.
Figure 11.2: Emergency management structure in Iowa

Source: Adapted from Iowa Homeland Security. (n.d.). Emergency management structure in Iowa. Retrieved from http://www.iowahomelandsecurity.org/about_HSEMD/EM_structure.html
How does the organizational structure of Iowa's HSEMD help it to plan for and respond to emergencies within the state?
While relatively new, Iowa's emergency management system is well designed. It operates 13 separate programs focused on protecting the health and well-being of its residents. Some of these programs include a Citizen Corps, Critical Infrastructure team, E-911 system, School Safety Program, and Threat Information and Infrastructure Protection Program.
Today, Iowa is still forward thinking in its protection efforts of its residents, as it has added terrorism to its responsibilities. The Threat Information and Infrastructure Protection Program works with the federal government to ensure the safety of public and private infrastructures in order to protect against the threat of terrorism or bioterrorism. Its Intelligence Fusion Center was developed post–9/11 to enhance efforts of information exchange to maintain public safety (Iowa Homeland Security, n.d.b). There are 72 fusion centers in the United States, one in each state and 22 in major urban areas. The Fusion Center in Iowa is at the capital, Des Moines.
Internal Disturbances and Mass Casualties
FEMA (2008) describes internal disturbances and mass casualty emergencies as riots, large-scale prison breaks, demonstrations or strikes that lead to violence, and acts of terrorism. The CDC (2013b) lists these types of emergencies in a similar manner, but adds bombings to its list. Probably the most vivid and current example of an emergency in this category is that of the April 15, 2013, Boston Marathon bombing. It was not only an emergency type "act of terrorism" as defined by FEMA, but it also involved mass casualties (which includes both injuries and deaths) as identified by the CDC. While the number of people affected by this incident was far less in comparison to the terrorist attacks of 9/11, this is still considered a mass casualty event because of the multitude of people affected, along with the potential for producing multiple deaths. According to a report from CNN (2013), three people died and nearly 200 people were injured when two pressure cooker bombs exploded near the finish line of the Boston Marathon. The bombing not only caused mass casualties, but it was also considered an act of terrorism, as news reports and the FBI would quickly discover.
Attacks and Bioterrorism
FEMA (2008) identifies these as nuclear, conventional, chemical, or biological warfare. The CDC (2013b) considers this category as terrorism with the use of biological agents and/or diseases such as anthrax or smallpox. The 2001 anthrax attacks following the terrorist attacks on 9/11 were considered this type of an emergency (Higgins et al., 2003). Other such emergencies on American land include the Revolutionary War (mainly along the East Coast states), the Civil War (nearly the entire nation), and World War II (Hawaii and the attack on Pearl Harbor) (British Battles, 2013; Civil War Talk, 2012; Naval History & Heritage Command, n.d.). As noted in Table 11.4, there have not been many of these attacks, especially bioterrorism events, in the United States in recent history.
Energy and Material Shortages
FEMA (2008) has identified these specifically as a unique emergency type, whereas the CDC does not have these listed among its emergencies. These are identified as strikes, price wars, labor problems, and resource scarcities (FEMA, 2008). A good example of this type of emergency occurred in the 1970s when gasoline shortages struck the nation. The Federal Power Commission had the authority to regulate the prices of natural gas sold to interstate pipeline companies (Breyer & MacAvoy, 1973). Apparently, the price wars prompted a nationwide gasoline shortage in both 1973 and 1979, causing long lines at the pump and product rationing. Interestingly, the maximum speed limit was reduced to 55mph to conserve gas, and, in order to further cut energy consumption, daylight savings time was introduced beginning in 1974 (Myre, 2012). Because of the Arab oil embargo, President Richard Nixon signed The Emergency Daylight Saving Time Energy Conservation Act of 1973 into law on January 6, 1974, in an effort to conserve energy during the winter months (The American Presidency Project, 2013). It was estimated to save an equivalent of 150,000 barrels of oil a day (The American Presidency Project, 2013). The concept was that by adding more hours of light each day, consumption of electricity for lamps and even stereos would drop. An early report from the United States Department of Transportation found that national electricity usage dropped by about 1% during daylight savings time (Harris, 2013).
Recent Outbreaks and Incidents
The CDC (2013b) identifies these as various disease outbreaks such as influenza. It classifies hurricanes in this category as well as in the natural disasters section. An example of such an emergency was the 2010 outbreak of Salmonella from infected eggs distributed across 14 states: Arkansas, California, Iowa, Illinois, Indiana, Kansas, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, Texas, and Wisconsin (CDC, 2013b). The outbreak started on May 1 and ran through November 30, infecting approximately 2,000 people with Salmonella. Epidemiologists investigated reports of illnesses in 11 states and identified 29 different restaurants who had served the infected eggs, which were traced back to two Iowa farms: Wright County Egg of Galt, Iowa, and Hillandale Farms of New Hampton, Iowa (CDC, 2013b).
Now that we've outlined the types of disasters that have occurred in the United States, we will move on to the public health core functions and how they interact with the emergency preparations undertaken by our nation.
11.4 Public Health Core Functions and Emergency Preparedness
As we have stated previously, there are various agencies at all levels of government that play a role in emergency response and preparedness. While each agency has its own specific role, they all work under the grand schematic outlined by the Department of Homeland Security.
Core Functions
For public health organizations, the key functions remain assessment, policy development, and assurance. Yet, in the public health role of emergency preparedness, these three elements are intertwined with the essential public health services, which we discussed in Chapter 1. However, all services provide the foundation for what public health organizations and professionals do to maintain the health and safety of the nation's population
Monitor health status to identify and solve health problems (CDC, 2010a). Under this service, emergency response teams at various levels of government, as well as nongovernmental agencies, monitor the activities surrounding potential harms to the United States. The harms under surveillance include threats of terrorism, as well as weather and natural disasters. For example, the FDA is charged with ensuring that our food is not only safe from bioterrorism threats, but is also grown free of disease and safely prepared for distribution (FDA, 2012). In addition, man-made crises—such as explosions or oil spills—are also protected under public health monitoring systems. Through the Occupational Safety and Health Administration, regular monitoring of safe conditions at various worksites maintains not only the health of the employees, but also of the local community as well (United States Department of Labor, n.d.).
Diagnose and investigate health problems and hazards in the community (CDC, 2010a). The most common example of diagnosing and investigating community health is through the annual influenza tracking system. The CDC tracks and investigates disease outbreaks, maps areas of high risk, and provides vaccines for protection. In the event of a bioterrorism attack, the CDC's role is the same, yet it performs emergency actions. It investigates the toxic pathogen and works quickly to secure an antidote (CDC, 2010a). For example, the CDC maintains a stockpile of vaccines against smallpox, known to be a possible bioterrorism weapon (CDC, 2001a). This essential service is considered part of the assessment role provided by public health. Through diagnosing the scope of a disaster, as well as investigating the health issues surrounding the disaster, public health officials tap into their role of assessment.

Gamma-Rapho via Getty Images
Communication efforts are one of the CDC's chief concerns in an emergency situation. Consistent, measured feedback is necessary to keep the public calm and informed.
Inform and educate the population regarding health issues and emergencies (CDC, 2010a). One of the most important issues during a crisis is obtaining factual information and communicating it effectively. People have an urgent need to know what is going on in the midst of a crisis. If left to their own thoughts and ideas, people could cause widespread panic. In order to combat this, the CDC sets up a command center specifically in times of crises that may prove detrimental to human health (Courtney, Cole, & Reynolds, 2003). Risk communications in times of crisis fall on a short timeline. Consideration must be taken to accurately inform, not make false claims; to calm, not panic; and to protect the people and investigation, not interfere. In the event of a terrorist attack, our nation's public communication systems are monitored. Too much information could breach the nation's security, but too little information could cause mass panic. The job of informing and educating during emergency times is difficult, yet the CDC does have solid protocols in place to provide necessary information to protect the public (Courtney, Cole, & Reynolds, 2003). Those communications vary depending on the emergency. For example, during the 2001 anthrax attacks, the CDC was charged with the communications efforts, receiving nearly 800 inquiries from news reporters that week (Robinson & Newstetter, 2003). In the following month, they handled an average of 900 calls from the media for updates (Robinson & Newstetter, 2003).
Mobilize teams into action to resolve the issue (CDC, 2010a). In the event of an emergency, teams are dispatched not only to provide communications support, but also for epidemiological support for investigative purposes. Remember, epidemiology is the science that studies the determinants of health among a population (United South & Eastern Tribes, Inc., 2009). One of the CDC's primary functions during emergencies involves dispersing public health resources (CDC, 2001a). In the 2001 anthrax scares, the CDC sent not only teams of medical personnel and epidemiologists to the scene, but also supplies of vaccines and other medical resources to assist with the crisis (Malecki et al., 2001; Polyak et al., 2002).
Develop policies and plans that support community health efforts (CDC, 2010a). Emergencies often require quick thinking. Sometimes, protocols must adapt to the crisis at hand, which was the case for the anthrax scare of 2001. Several work practices were reevaluated and staff roles redefined at the CDC following the efforts of the 2001 anthrax attacks (Robinson & Newstetter, 2003). This example reflects this particular public health service in action, as it prompted the development or revision of policies. Policies are often developed because of poor responses or failed attempts at successful emergency preparedness. This essential service is considered part of the policy development role of public health. Through modifications of plans and the development of new and improved policies following disasters, public health officials fulfill their role as policy developers.
Enforce the laws and regulations to protect the public's health (CDC, 2010a). In national emergencies, the lead agency is the Office of Homeland Security. The public's health is the most important element of this agency. Through the laws and regulations set forth by this agency under the rules of the Stafford Act, the public's health and safety is protected (FEMA, 2007). An example of enforcement activities could be seen during the Boston Marathon bombings in 2013. The Office of Homeland Security took charge of the incident, utilizing agents from the FBI to coordinate the activities. One of the two men accused of the attack was arrested under the rules and regulations under the FBI, working in conjunction with homeland security agents. (The other was killed in a shootout with police.)
Link people to health services and ensure that they receive care (CDC, 2010a). This works in conjunction with the fourth public health service of mobilizing teams into action. The CDC, in conjunction with state and local health agencies, ensures that medical help and other services are accessible and available during an emergency (Malecki et al., 2001; Polyak et al., 2002).
Ensure competent public and personal health care workforce (CDC, 2010a). As part of their emergency response preparedness, public health agencies (particularly the CDC) require extensive training of their workforce (Courtney, Cole, & Reynolds, 2003). Practice exercises and mock drills help assure the public that personnel will be ready and able to handle most crises—at the state and national levels (Courtney, Cole, & Reynolds, 2003; Robinson & Newstetter, 2003). Because of this commitment to training, the CDC and other public health agencies that are dispatched during an emergency will be competent in their subsequent crisis responsibilities. The most recent training course developed by the CDC is known as CDCynergy, a communications-specific course that teaches emergency responders how to prepare for crisis communications (CDC, 2010b). Furthermore, the CDC routinely offers online or on-site training relating to various emergencies, such as risk management, emergency preparedness, and law and ethics during emergencies (CDC, 2013b). This essential service is considered part of the assessment role provided by public health services. By building a competent team of public health professionals—particularly adept to emergency services—this fulfills public health's third main function of assurance.
Evaluate effectiveness of the personnel and services offered to the public (CDC, 2010a). As you've learned throughout the text, evaluation is an important part of public and community health. Whether developing a program or assessing needs, or responding to an emergency, public health officials must evaluate their effectiveness in order to serve the public in the most effective manner. In emergencies, the evaluation takes place following the crisis or mock exercise. In most cases, lessons learned from past events have shaped the manner in which response occurs in the future (Robinson & Newstetter, 2003). This evaluation provides feedback and support for the changes or development of policies to improve public health's effectiveness.
Research for new insights and innovative solutions to health problems. As we've mentioned earlier, the Office of Counterterrorism and Emerging Threats (OCET), operating under the FDA, facilitates the development of safe and effective medical countermeasures in the event of a terrorist or bioterrorist attack (FDA, 2012). The FDA has extensive research facilities where it focuses on countering acts of terrorism. In addition, the Department of Homeland Security is also researching new insights and solutions to combat terrorism. For natural disasters and man-made disasters, preparations from Occupational Safety and Health Administration (OSHA) and FEMA continuously aim for improvements and new methods for coordinating response and relief efforts (FEMA, 2008; United States Department of Homeland Security, n.d.; United States Department of Labor, n.d.).
The National Incident Management System (NIMS)
This system is considered one of the world's leading management systems for monitoring and protecting populations (Lester & Krejci, 2007). NIMS was originally issued on March 1, 2004, by the Department of Homeland Security in order to provide consistent management across all governments during emergencies of a national scope (United States Department of Homeland Security, 2008). Throughout its use in times of disaster, it has undergone numerous revisions for clarification, enhancements, and improved response. The most recent document revision was approved in 2008 and includes additional details on eliminating redundancy, expanding intelligence roles, clarifying the role of the incident command system (ICS), and emphasizing teamwork among all agencies (government and nongovernment) for the benefit of the general public (United States Department of Homeland Security, 2008).
By design, NIMS is a proactive approach to guide all emergency crews—public and private—in an effective manner. The United States Department of Homeland Security (2008) defines the system as a means of working "seamlessly to prevent, protect against, respond to, recover from, and mitigate the effects of incidents, regardless of cause, size, location, or complexity" (p. 13). Basically, NIMS is the blueprint that all emergency personnel will follow in the event of a disaster. It provides the specific processes that incident management personnel must follow. Refer to Table 11.5 for an overview of the system.
The system was built following the 9/11 attacks as part of the responsibilities of national protection. While the response to 9/11 was never condemned, there were behind-the-scenes incidents that prompted the need for a significant strategic system to guide emergency workers and volunteers during times of disasters. This coordination involves both private and public organizations, as well as governmental agencies that respond to emergencies. Unfortunately, when put into action, the system failed miserably, as noted after Hurricane Katrina. See Case Study: Hurricane Katrina: A NIMS Failure for further discussion.
| Table 11.5: Overview of NIMS | |
| What NIMS Is | What NIMS is NOT |
| A comprehensive, nationwide, systematic approach to incident management, including the incident command system, multiagency coordination systems, and public information | A response plan |
| A set of preparedness concepts and principles for all hazards | Only the incident command system or an organization chart |
| Essential principles for a common operating picture and interoperability of communications and information management | A communications plan |
| Standardized resource management procedures that enable coordination among different jurisdictions or organizations | Only applicable to certain emergency management/incident response personnel |
| Scalable, so it may be used for all incidents (from day-to-day to large-scale) | Only used during large-scale incidents |
| A dynamic system that promotes ongoing management and maintenance | A static system |
| Source: Directly quoted from the United States Department of Homeland Security (2008). | |
NIMS contains five main components: preparedness, communications and information management, resource management, command and management, and ongoing management and maintenance (USDHS, 2008).
Component 1: Preparedness: This component describes the measures that should be developed and incorporated into preparedness programs to enhance overall preparedness for all response activities. This component is aimed at organizations such as fire and police departments, public health entities, governmental agencies, and business and corporations for emergencies, and focuses on national policy to identify and prioritize critical infrastructure and key resources to prevent and mitigate effects of emergencies.
Component 2: Communications and Information Management: This component focuses on the application of flexible communications and information systems that will work seamlessly during an emergency. It stresses the development of procedures that are interoperable, reliable, scalable, portable, and resilient. The system recommends that communities build an emergency communications system that gathers all necessary information (traffic, weather, damage, resources, etc.) for decision making and public dissemination.
Component 3: Resource Management: Effective deployment of personnel and supplies is necessary in times of emergency, and managing the distribution of such resources needs proper planning to be quick and efficient for the public's health and safety. Such resources include medical supplies and vaccines, as well as basic survival items such as food and water. Systems need to be in place to manage these resources in the event of a disaster, from the local level to the national scene. National resources include transportation, medical care, search and rescue, food and water, energy, animal and agricultural issues, and volunteers and donations.
Component 4: Command and Management: Not every person can be in charge, therefore the importance of development of a command and management center is critical at the local, state, and national levels. This component of NIMS provides the basis for establishing an incident command system (ICS). An ICS is much like an organizational chart, providing details as to which entity reports to which entity. Within each entity is another organizational chart that lists the chain of command. In essence, the largest national emergencies are led by the president of United States. At the local level, that person could be the mayor, or fire chief, or whoever is designated by the emergency plan. ICS is based on 14 management characteristics: common terminology, modular organization, management by objectives, incident action planning, manageable span of control, incident facilities and locations, comprehensive resource management, integrated communications, establishment and transfer of command, chain of command/unity of command, unified command, accountability, dispatch/deployment, and information/intelligence management. Each of these roles is outlined within the NIMS document.
Component 5: Ongoing Management and Maintenance: This component focuses on two sections, the National Integration Center (NIC) and Supporting Technologies. The NIC was established to provide ongoing management and maintenance for NIMS. The NIC is responsible for collecting and analyzing all potential revisions to NIMS and also for leading the development of training and exercises to enhance NIMS's overall effectiveness. Supporting Technologies focuses on research and development of the various science practices and technologies that may enhance and improve NIMS. This includes improvements in communications, monitoring, response, and mitigation.
Case Study: Hurricane Katrina: A NIMS Failure
One year after its implementation, NIMS was tested under the disaster area left behind due to Hurricane Katrina.

Air Force Public Domain/Science Faction/SuperStock
The effects of Hurricane Katrina tested the nation's ability to manage emergency response efforts between state and federal agencies.
Storm Overview
The weather system first developed over the Bahamas as a tropical storm on August 24, 2005, at which time it was given the name Tropical Storm Katrina. The National Weather Climate Data Center (a branch of the National Oceanic and Atmospheric Administration [NOAA]) had largely predicted that the storm would become a major hurricane and make landfall in the central part of the Gulf of Mexico. On August 25, the system became a Category 1 hurricane, which had sustained winds of 74 miles per hour. It crossed over the southern tip of Florida between Hallandale Beach and North Miami Beach with wind speeds at 80mph. The next day, Katrina became a Category 3 hurricane with sustained winds of 125mph as it continued to strengthen, moving over the warm waters of the Gulf. As the system moved through the Gulf, it grew into a Category 5 hurricane (the highest category on the Saffir–Simpson scale, with sustained winds of at least 170mph). Eventually, the hurricane dropped back to a Category 3 before it struck the shores of the Gulf Coast over New Orleans. For at least a day before making landfall, the storm's rain and winds were felt across the Gulf Coast from the panhandle of Florida to the southwestern coastal areas in Louisiana. Katrina made landfall on Monday, August 29, when more than an inch of rain per hour fell for 3 consecutive hours, then slowed to a half-inch per hour for the next 5 hours. It was estimated that more than 10 inches of rain fell over southeastern Louisiana and southwestern Mississippi during the course of the storm as it approached, made landfall, and retreated up the mid-Atlantic states.
Storm Overview Source: National Oceanic and Atmospheric Administration (2012).
Actual Disaster Management
When the system first became a hurricane (at Category 1), FEMA mandated an evacuation of several coastal areas in Louisiana. That same day, Louisiana Governor Kathleen Blanco called on 4,000 National Guard troops to assist. The following day, all of New Orleans was alerted to a mandatory evacuation. Also that day, the Superdome (the stadium that is home to the New Orleans Saints pro-football team) became an emergency shelter for those who either had no means of evacuating or refused to leave. It was estimated that approximately 22% (about 100,000 people) of the 458,000 New Orleans population did not evacuate, with about 20% of those 100,000 people relocating to the Superdome. The remaining 80% stayed in their homes or other locations.
At the Superdome: Generators allowed limited lighting of the arena, but there were no other amenities. With no operational restrooms or subsequent alternatives, the facility quickly overflowed with human urine, feces, and garbage. In addition, there was no food, water, or medical supplies.
At the Convention Center: Emergency crews rescued stranded residents from rooftops and attics, transporting them to the center. Much like the Superdome, the Convention Center lacked water, food, medicines, and utilities. Eventually, conditions at the Center became similar to conditions at the Superdome.
In Hospitals and Nursing Homes: Patients and staff members were stranded without power or other vital services. Conditions were grim as places ran out of food, water, and medicine.
On the Streets: New Orleans looked like a war zone, only not from gunfire or explosions but from flooding and high winds. Dead bodies could be seen floating down flooded streets. Many people drowned at home because they were too frail to evacuate or move to higher ground. Bodies were found drowned in attics, the highest place they could possibly go. As a result of failure/inability to evacuate, one nursing home lost 35 elderly patients.
At the Houston Astrodome: As conditions were obviously uninhabitable at both the Convention Center and the Superdome, Houston opened its doors to evacuees starting about 5 days after the Hurricane hit. By the end of the day on September 3, both facilities in New Orleans were evacuated to Houston.
Actual Disaster Management Source: Brinkley (2006).
NIMS Failure
The true test of the system, which looked effective on paper, occurred during Katrina. One of the most dominating features of the failure occurred midcrisis when NIMS inadequately handled leadership and authority concerns. Sometime during the search and rescue, operations halted because the federal government stepped in to take control. At that time, the states and local parishes were well organized in their recovery efforts and did not see the need to relinquish control. As a result, disaster relief and recovery efforts came to an abrupt halt until the "who's in charge" question was addressed. The federal government had claimed prime authority over the disaster, stating that it presented a threat to national security. Once authority was lost, states would have a difficult time regaining control, and hence the battle for situational control began. While it should have provided guidance on authority lines as well as chain-of-command procedures, NIMS did not address these issues. It had only suggested that collaboration should be employed in times of emergencies, but clearly did not outline the best practices. Historically, states and local governments have done well to take care of their own in times of disaster—with aid and assistance through the federal government, not overall control.
Research of the NIMS system found that this lack of leadership left the wounded city of New Orleans in the aftermath of the devastation longer than necessary. This significant NIMS shortfall is likely what caused the slowing of rescue and recovery operations; inadequate food, water, and medical supplies for those sheltered in the Superdome and the Convention Center; and the sanitation deficiencies at all shelter locations. While the 2004 NIMS document called for a unified command with joint decision making, these concepts were either ignored or avoided during Katrina. It was the mass public (who were to be protected) that suffered, with thousands dying and even more wounded and sick.
Although it was this gross negligence of joint leadership that hurt the people within the city of New Orleans, it was also the impetus that prompted significant changes to NIMS. "NIMS has the potential to become an effective vehicle for promoting the change necessary within the collaborating organizations. NIMS can help provide an environment that stresses common interests and training toward truly collaborative decision making" (Lester & Krejci, 2007, p. 87).
NIMS Failure Source: Lester & Krejci (2007).
In addition to the core functions of public health, the emergency response teams also follow eight key principles and strive for accreditation, which provides a federal "nod of approval" that an organization or entity is prepared and willing to act in the event of an emergency. We will now discuss these principles and associated accreditation standards. Furthermore, this next section will also review the past and current alert system for terrorism attacks, which emergency response teams must understand as they prepare for such disasters.
11.5 Principles of Emergency Response and Preparedness
In its many emergency response and preparedness training programs, FEMA provides extensive details on handling emergencies at every level, from the individual to the federal government. Some of the key benefits of such training is empowering individuals—emergency management personnel, communities, and organizations—to develop an emergency response and preparedness plan, the best defense for successful tackling of disasters. While NIMS is considered a best practice system that is utilized by national, state, and local governments, its foundations came through FEMA training programs, including its independent study course "Fundamentals of Emergency Management" (FEMA, 2011).
One of the most critical pieces of managing an emergency revolves around the planning for one. FEMA (or the role of FEMA) has existed for more than 2 centuries, evolving into the nation's most knowledgeable entity on emergency preparation, management, response, and recovery. In this section, we will discuss the principles of emergency management along with the importance of accreditation for emergency management agencies.
Eight Principles of Emergency Management
In 2007, FEMA's Emergency Management Institute's Higher Education Project agreed upon eight specific principles for emergency management that are now used to develop a doctrine for emergency management personnel. These principles are outlined in Spotlight: Principles of Emergency Management.
Spotlight: Principles of Emergency Management
Comprehension: Consider and take into account all hazards, all phases, all stakeholders, and all impacts relevant to disasters.
Progressive: Anticipate future disasters and take protective, preventive, and preparatory measures to build disaster-resistant and disaster-resilient communities.
Risk-driven: Use sound risk-management principles (hazard identification, risk analysis, and impact analysis) in assigning priorities and resources.
Integrated: Ensure unity of effort among all levels of government and all elements of a community.
Collaborative: Create and sustain broad and sincere relationships among individuals and organizations to encourage trust, advocate a team atmosphere, build consensus, and facilitate communication.
Coordinated: Synchronize the activities of all relevant stakeholders to achieve a common purpose.
Flexible: Use creative and innovative approaches in solving disaster challenges.
Professional: Value a science-and knowledge-based approach based on education, training, experience, ethical practice, public stewardship, and continuous improvement.
Source: FEMA (2011).
Principle 1: Comprehension
The International Association of Emergency Managers (IAEM) (2007) notes that understanding all types of emergencies will help agencies better prepare for what damages and harms could occur. This consists of four specific components: hazards, phases, impacts, and stakeholders. All hazards must be reviewed and treated independently, including biohazards, natural harms, and terrorism. "Treating all hazards the same in terms of planning resource allocation ultimately leads to failure" (IAEM, 2007, p. 5). The four comprehension phases are mitigation, preparedness, response, and recovery (IAEM, 2007). Regarding impact, emergency managers must review not only human impact, but environmental and infrastructure impact. Key stakeholders not only include the emergency response teams and agencies but also potentially affected businesses, individuals, and the general public.
Principle 2: Progressive
Research and disaster surveillance shows that disasters are becoming more frequent and far more common (IAEM, 2007). Emergency preparedness and response must not remain stagnant in its preparations and response. Continuous planning, drills, and exercises will enable disaster response to be more progressive rather than reactive moving forward. As an example, climate change includes warmer, wetter, and more unstable atmospheric pressure (Bergholt & Lujala, 2012). Some researchers believe that the rising temperatures and volatile atmospheric conditions are directly related to increasing storm severity and frequency in hurricanes, floods, and fires (Bergholt & Lujala, 2012).
Principle 3: Risk-Driven
Every community in the United States has a different risk level. For urban areas, the risks are greater for human life and infrastructure; in rural areas, the risks are greater for agriculture and environment. Regardless of the risk, emergency management preparedness personnel must review and understand the risks across the nation. This requires setting policies and priorities that are based upon risks to lives, property, and the environment (IAEM, 2007).
Principle 4: Integrated
The focus on integration revolves around aligning the goals and objectives of response among all emergency responders, the communities, and the stakeholders. According to the IAEM (2007, p. 6), "Unity of effort is dependent on both vertical and horizontal integration." In brief, local emergency response programs must be aligned with the state; and state programs must be aligned with federal programs. When all local programs are integrated within a community, there is horizontal integration. When local, state, and federal integrate, there is vertical integration. Full integration will provide increased protection and quicker recovery efforts in the event of an emergency because every responder will understand and know his or her role in an emergency.
Principle 5: Collaborative
Collaboration works in conjunction with integration in that individuals, local governments, state governments, and federal emergency management personnel work together and succinctly for one purpose: to mitigate the emergency and assist those affected by it as defined by their specific role. This approach ensures a smooth transition from the status quo to optimal emergency response. The best advice for this principle can be summed up by a statement from Mr. Michael D. Selves in an oral testimony before the United States House Subcommittee on Emergency Management of the Committee on Transportation and Infrastructure: "If we shake hands before a disaster, we won't have to point fingers afterwards" (IAEM, 2007, p. 8).
Principle 6: Coordinated
All activities surrounding emergency response and planning must be synchronized at all levels to insure a smooth outcome (IAEM, 2007). This involves elements including planning, response, recovery, and communications.
Principle 7: Flexible
With the increased number and types of disasters occurring in the United States, all emergency management teams must be flexible in their plans and responses. The most obvious phase for flexibility comes with response (IAEM, 2007). Responding to natural disasters, such as hurricanes and tornadoes, requires a certain type of organization; yet, responding to a terrorist attack of unknown proportions requires team flexibility as information becomes available.
Principle 8: Professional
This principle points toward acting and responding in a professional manner before, during, and after an emergency. It focuses on five key elements: code of ethics, professional associations, board certification, specialized body of knowledge, and standards and best practices. The IAEM (2007) stresses each of these elements for emergency management personnel in its training programs.
Emergency Management Accreditation Program (EMAP)
Also as part of the fundamentals of emergency management is the Emergency Management Accreditation Program (EMAP). This program provides standards for processes used in emergencies such as prevention, mitigation, preparedness, response, and recovery (FEMA, 2013). It provides accreditation to organizations (such as fire departments, hazardous materials teams, police departments, and health departments) operating with a set of standards that have been developed as "best practices" for preparing for and responding to disasters. Through this accreditation process, the intent is for emergency management groups to focus on the same principles; thus, making collaboration and cooperation more evident in the event of a disaster. FEMA (2013) notes that these standards for accreditation address the following areas:
Program management
Administration and finance
Laws and authorities
Hazard identification, risk assessment, and consequence analysis
Hazard mitigation
Prevention and security
Planning
Incident management
Resource management and logistics
Mutual aid
Communications and warning
Operations and procedures
Facilities
Training
Exercises, evaluations, and corrective action
Crisis communications, public education, and information.
The Department of Homeland Security Advisory System (2002–2011)
In an effort to easily and quickly disseminate threats or a risk of a threat to all levels of government as well as to the American people, the United States Department of Homeland Security (n.d.) devised a color-coded system of alerts known as the DHS Advisory System (after 2011, the system became known as the National Terrorism Advisory System [NTAS]). Established in March 2002, the alert system was fairly simple and provided a unified message for threats or potential dangers:

AFP/Getty Images
Homeland Security Chief Tom Ridge explains the DHS Advisory System on March 12, 2002. The five levels were replaced by a three-level system in 2011 in order provide a more clear-cut feedback mechanism to the public.
Green—Low condition of threat. This told the nation that there were no imminent threats to the nation. For homeland security personnel, it meant that training and protective planning continues as usual.
Blue—Guarded condition of threat. This meant that there was a general risk of a terrorist attack and that emergency response procedures should be updated and reviewed. Public communications were outlined and utilized as necessary.
Yellow—Elevated condition of threat. This indicated that there was a significant risk of a terrorist attack, and surveillance of critical locations would increase along with implementing emergency response plans, when necessary.
Orange—High condition of threat. This level noted that there was a high risk of terrorist attacks. Security efforts with the military and law enforcement would ensue and preparations for relocation of citizens would commence.
Red—Severe condition of threat. This indicated a severe risk of a terrorist attack and that NIMS would be put into effect. This includes dispatching emergency response teams to specific sites as well as closing public and government facilities, and working to address critical emergency needs such as medical aid.
The National Terrorism Advisory System (2011–Present)
On April 20, 2011, Secretary of Homeland Security Janet Napolitano announced that the National Terrorism Advisory System (NTAS) had been revised to provide a more credible and clear mode of public communications on terrorism (United States Department of Homeland Security, 2011).
Rationale Behind the Changes
The new system provides a more timely and effective means of alerting the public to credible terrorist threats by using only three specific levels rather than the five levels in the color-coded system. According to the Homeland Security Advisory Council's Task Force on the advisory system, the color-coded system was confusing in that it was difficult to ascertain the differences between "guarded" at the blue level or "elevated" at the yellow level, and "high" at orange versus "severe" at red (Homeland Security Advisory, 2009). The task force noted in its report that "there is a disturbing lack of public confidence in the system" (Homeland Security Advisory, 2009, p. 2).
The report also noted that in this post–9/11 era, there will never be a condition in the United States where the threat level will fall below "guarded" (Homeland Security Advisory, 2009). Thus, the norm will be considered "guarded" with three new levels being created whose meanings are clearly defined and outlined.
The New Advisory System
Considering that the United States will remain on "guarded" status under normal conditions, the Office of Homeland Security will only issue an alert when a threat is possible and credible. These alert levels are shown in Table 11.6.
| Table 11.6: New NTAS alert system | |
| Threat Level | Interpretation |
| Imminent Threat | Warns of a credible, specific, and impending terrorist threat against the United States. This is the highest level in the new system and indicates that there is information on timing and location of the threat. |
| Elevated Threat Alert | Warns of a credible terrorist threat against the United States. This indicates there is a credible threat, but no specific information is available on timing or location. |
| Sunset Provision | An individual threat alert is issued for a specific time period and then automatically expires. It may be extended if new information becomes available or the threat evolves |
| Source: United States Department of Homeland Security (2011). | |
According to the United States Department of Homeland Security (2011), the alerts will provide the public with a summary of the threat, information to help with public safety initiatives, and steps that communities and individuals should take to prevent or respond to the pending threat. It is important to note that some threats will only be released to law enforcement or areas that could be affected by the pending threat.
The alerts will be issued through state and local entities as well as the media and public broadcasting stations. In addition, the NTAS system posts its alerts on its website as well as two social media outlets: Facebook and Twitter (United States Department of Homeland Security, 2011).
11.6 Bioterrorism Preparedness
There is not much difference for public health professionals in preparing for an emergency and preparing for bioterrorism. From the public health perspective, the preparedness for bioterrorism lies in ensuring the amount and availability of an antidote or vaccine. In addition, distribution methods are also part of this preparation.
Biological Agents
Section 11.1: Introduction defined the term bioterrorism and outlined the chemical and biological agents associated with this type of emergency. Table 11.7, compiled from the CDC (2013n.d.), is a complete list of the specific agents the CDC has identified that could potentially harm the United States.
| Table 11.7: Bioterrorism biological agent categories |
| Category A |
| High priority agents that pose the highest national security risk |
| Anthrax (Bacillus anthracis) |
| Botulism (Clostridium botulinum toxin) |
| Plague (Yersinia pestis) |
| Smallpox (variola major) |
| Tularemia (Francisella tularensis) |
| Viral hemorrhagic fevers (filoviruses [e.g., Ebola, Marburg] and arenaviruses [e.g., Lassa, Machupo]) |
| Category B |
| Second highest for national risk security breaches |
| Brucellosis (Brucella species) |
| Epsilon toxin of Clostridium perfringens |
| Food safety threats (e.g., Salmonella species, Escherichia coli O157:H7, Shigella) |
| Glanders (Burkholderia mallei) |
| Melioidosis (Burkholderia pseudomallei) |
| Psittacosis (Chlamydia psittaci) |
| Q fever (Coxiella burnetii) |
| Ricin toxin from Ricinus communis (castor beans) |
| Staphylococcal enterotoxin B |
| Typhus fever (Rickettsia prowazekii) |
| Viral encephalitis (alphaviruses [e.g., Venezuelan equine encephalitis, eastern equine encephalitis, western equine encephalitis]) |
| Water safety threats (e.g., Vibrio cholerae, Cryptosporidium parvum) |
| Category C |
| While still potent, these agents have the lower priority among the biological weapons. |
| Emerging infectious diseases such as Nipah virus and hantaviruses |
| Source: Centers for Disease Control and Prevention (n.d.). |
Chemical Agents
Like their biological counterparts, chemicals can also pose potential harms to human life and the environment. See Table 11.8 for a partial list of these agents.
| Table 11.8: Bioterrorism chemical agents | |
| Albrin | Mercury |
| Adamsite (DM) | Methyl bromide |
| Ammonia | Methyl isocyanate |
| Arsenic | Mustard gas (H) |
| Arsine (SA) | Nicotine |
| Barium | Nitrogen mustard |
| Benzene | Opioids |
| Brevetoxin | Osmium tetroxide |
| Bromine | Paraquat |
| Bromobenzylcyanide (CA) [Riot control agent] | Phosgene (CG) |
| BZ | Phosgene oxime (CX) |
| Carbon Monoxide | Phosphine |
| Chlorine (CL) | Phosphorus—elemental, white, or yellow |
| Chloroacetophenone (CN) [Riot control agent] | Potassium cyanide (KCN) |
| Chlorobenzylidenemalononitrile (CS) [Riot control agent] | Ricin |
| Chloropicrin (PS) [Riot control agent] | Sarin (GB) |
| Chromium | Saxitoxin |
| Colchicine | Selenium |
| Cyanide | Sodium azide |
| Dibenzoxazepine (CR) [Riot control agents] | Sodium cyanide (NaCN) |
| Digitalis | Sodium monofluoroacetate (compound 1080) |
| Distilled mustard (HD) | Soman (GD) |
| Ethylene glycol | Stibine |
| Fentanyls and other opioids | Strychnine |
| Hydrazine | Sulfuryl fluoride |
| Hydrofluoric acid | Tabun (GA) |
| Hydrogen chloride | Tetrodotoxin |
| Hydrogen cyanide (AC) | Thallium |
| Hydrogen fluoride (hydrofluoric acid) | Trichothecene |
| Lewisite | VX |
| Source: Centers for Disease Control and Prevention (2013b). | |

© Bettmann/Bettmann/Getty Images
A Vietnamese mother holds her daughter, believed to have been deformed through her father's exposure to Agent Orange during the Vietnam War.
While there is little in the news on chemical use in terrorist acts, it is still a possibility that the CDC takes very seriously (Khan, Levitt, & Sage, 2000). Chemical weapons are not as common as the biological ones because biological weapons often are undetectable in their early stages. Thus, significant harm could occur long before the infectious agent is detected. However, chemical weapons are still utilized, as in the 1995 attack in the Tokyo subway system (Rivera, n.d.). Liquid sarin, which was developed in the 1930s by Nazi Germany, was released in the busy subway. The terrorists filled plastic bags with sarin and punctured them to release the toxin, killing 12 people and injuring more than 6,000 (Rivera, n.d.).
There are no major incidents of chemical toxins used in attacks in recent U.S. history, but probably the most commonly known chemical warfare use was during Vietnam by the United States Air Force with the substance code-named "Agent Orange." Its chemical name is 2,3,7,8-tetrachloro-dibenzo-para-dioxin, or TCDD, but it is basically a combination of herbicides used to destroy foliage in Vietnam to uncover hidden enemy troops (Aspen Institute, 2011). While it did what it was intended, it had the consequence of sickening thousands of troops on both sides (United States and North Vietnam), as well as causing civilian issues such as fetal defects, miscarriages, and neurological illnesses (Aspen Institute, 2011). Our nation is still handling health concerns from Vietnam veterans. Review Case Study: Public Health Response to Agent Orange for more details on the public health response to Agent Orange.
Case Study: Public Health Response to Agent Orange
Immediately following the Vietnam veterans' return to the United States, claims of diseases and deaths arose in alleged connection to the use of Agent Orange (TCDD). Initially, the CDC responded to significant pressures regarding exposure of troops to the chemical agents. Two studies were conducted to investigate the toxicity of TCDD in veterans (CDC Veterans Health Studies, 1988). Of the 979 eligible veterans who were exposed and eligible for the study, 900 (92%) participated in this research. Part of the research methods included a blood analysis as well as an interview questionnaire. This was the first-ever research on the exposure of Agent Orange to U.S. troops that looked into the potential harm to large segments of that population. The results found that "except for two veterans who had levels greater than 20 ppt, current serum TCDD levels in this study are essentially the same in the Vietnam veterans and the comparable group of veterans who did not serve in Vietnam. It seems, therefore, that most U.S. Army ground combat troops who did not handle or spray herbicides were not heavily exposed to TCDD in Vietnam" (CDC Veterans Health Studies, 1988, p. 1254).
Over the years and decades that followed, continuing analysis of veteran illnesses seemingly debunked the study. Many claimed faulty science or misinterpretations (Gough, 1991) and members of the U.S. public health community eventually responded to public outcry that their own government had poisoned their military troops. A study performed in 2011 did offer some significant support that Agent Orange caused a plethora of health issues for troops serving during the Vietnam War (Young & Cecil, 2011).
Eventually, the Veteran Administration developed a stance that approached the diseases developed from exposure to Agent Orange as "presumptive diseases" because of their exposure during military service (United States Department of Veteran Affairs, 2013). In addition, the VA acknowledged the issue and is now providing disability compensation and survivor benefits for those who had noted exposure to Agent Orange (United States Department of the Veteran War Affairs, 2013).
Illnesses From Agent Orange
Exposures to Agent Orange have been connected to the following illnesses:
AL Amyloidosis (a rare disease that affects tissues and organs)
Chronic B-cell leukemias
Chloracne (skin conditions similar to acne but disabling)
Diabetes mellitus type II
Hodgkin's disease
Ischemic heart disease
Multiple myeloma
Non-Hodgkin's lymphoma
Parkinson's disease
Peripheral neuropathy
Porphyria Cutanea Tarda (liver dysfunction by thinning and blistering of the skin)
Prostate cancer
Respiratory cancers
Soft tissue sarcomas (cancer within body tissues)
Source: United States Department of Veterans Affairs (2013)
Furthermore, the use of Agent Orange damaged the entire country of Vietnam. The chemical seeped into soils, contaminating the country's food supply for both humans and animals. In other words, the ecosystem of Vietnam became contaminated after the use of TCDD (Palmer, 2007). Although the substance hasn't been used for more than 30 years in Vietnam, its effects are still seen in present-day Vietnam. In 2012, cleanup efforts of the country began with the assistance of the United States and should be complete by 2016 ("U.S. Begins," 2012).
Bioterrorism and Ethics
There are two areas of ethics that revolve around bioterrorism. The first is the ethical manner in which public health responds to acts of bioterrorism, and the second regards the research that may actually promote bioterrorism.
Response and Bioterrorism
While it seems as though acts of bioterrorism would promote superior health care and public health attention, it does have its ethical challenges. In the world of health care, there are three critical responsibilities: detection, containment, and treatment (Wynia & Gostin, 2004). It is possible that detection might fail if people do not have access to care or do not understand that their symptoms are associated with an act of bioterrorism. Containment might fail if physicians treating those affected do not act quickly and effectively to reduce the spread of infectious diseases from bioterrorism acts. Finally, treatments may fail if there is no duty for providing health care in the event of an emergency.
Detection: This task revolves around public health's ability to monitor and perform adequate surveillance after an attack (Wynia & Gostin, 2004). These activities are generally discovered from reports through the health care system. If doctors or emergency rooms fail to report incidents—even just one—the possibility of the disease spreading could occur. The other detection issue revolves around access to care. Our nation has struggled with providing such easy access for its population, and thus, may be remiss at ensuring that bioterrorism threats are quelled quickly before they spread (Wynia & Gostin, 2004).
Containment: This task involves ensuring that appropriate measures are taken to reduce the risk of exposure to others. Public health often cannot contain an outbreak as rapidly as necessary (Wynia & Gostin, 2004). Without quick containment—either in the form of isolation or quarantine—the disease cannot be stopped from reaching epidemic proportions. Ethically speaking, there should be a stronger role in terms of information sharing between public health officials and medical practitioners to determine the fast containment of diseases from bioterrorism.
Treatment: Health care workers are the common second wave of infected persons in the event of a bioterrorism attack (Wynia & Gostin, 2004). At first, the medical team may not know what they are handling, and thus, contract the disease themselves. The Hippocratic oath requires physicians to treat all medical conditions, but the problem lies in the high cost of doing so in bioterrorism events. According to Wynia and Gostin (2004), some hospitals in New York City have announced that they will not accept victims of bioterrorism because of that very cost. Health care providers have a legitimate fear of contracting deadly diseases from those infected by bioterrorism agents, and the hesitation to treat is understandable. Historians note that fear caused poor medical treatments during the Black Plague and the more recent HIV epidemic (Wynia & Gostin, 2004). Furthermore, there were 57 reported cases from 1981 to 2010 in which health professionals who treated those with HIV actually contracted the disease (Beltrami et al., 2001; CDC, 2011). (Note: The CDC operates a voluntary reporting system for such cases; therefore, it is likely that there are far more cases than noted here.) The unethical decision to refuse treatment can be avoided with not only precautionary measures, but also with a stronger connection to the profession's code of ethics, which includes a duty to treat. In a case of bioterrorism, without treatment, many could perish; or worse, more could be infected and considerable deaths could ensue.
Research and Bioterrorism
Ideas for bioterrorism often stem from existing scientific research. For example, we have eradicated smallpox with a vaccine, but we can regenerate the disease to become much more deadly and resistant to vaccines. Hence, smallpox could be manufactured as a weapon. It has been suggested that some scientific studies, especially those surrounding genetics and the human genome, be kept under high guard because of the potential public health threat and national security breach (Selgelid, 2007).
According to a report from the Central Intelligence Agency (CIA) in 2003, biotechnology has the means of becoming the most deadly weapon because it could create a disease that would wipe out the population. So what should be kept secret, and what should be made public? Perhaps the more ethical dilemma is determining the continuation of biological research at all.
While our world desires research in this area in order to eradicate many infectious diseases that affect the populations around the globe, or perhaps stumble on a cure for cancer or AIDS, we must recognize that both allies and enemies will see the work. A meeting between the scientific world and security entities agreed upon a procedure that would reduce risk with such research (Selgelid, 2007). It contained four key elements, none of which strongly address the issue of reducing the publication of potentially harmful research. These are:
Scientific studies are submitted through a stringent peer-review process, which protects the integrity of the scientific community. It believes that without such rigorous processes, it would not be able to further advance biomedical research.
The scientific community recognizes the prospect of bioterrorism and understands that its published information may be abused when placed in enemy hands. The statement reads: "[W]e are committed to dealing responsibly and effectively with safety and security issues that may be raised by papers submitted for publication, and to increasing our capacity to identify such issues as they arise" (Selgelid, 2007, p. 39).
Scientific journals consider their appropriateness as to which papers are published, taking into consideration topic, design, and timeliness.
The scientific community recognizes that there may be times when potential dangers will outweigh the potential benefits from publication. It is committed to ensuring that published research will maximize the benefits and minimize risks of misuse.

© Brooks Kraft/Corbis Historical/Getty Images
Employees of the National Security Agency in Fort Meade, Maryland, are tasked with the responsibility of protecting any research that might prove potentially harmful.
Furthermore, Somerville and Atlas proposed an ethical code for research publication in 2005, but it was never adopted in the United States. In their proposal, Somerville and Atlas (2005) included a warning system for potentially harmful research and a censorship process to restrict detrimental biological studies from publication. Since then, many countries around the world have adopted modified versions of the Somerville and Atlas Code of Ethics for research in biotechnology in order to reduce or quell bioterrorism (Rapport, n.d.). The United States has yet to adopt one.
Experts have strongly recommended that policies be developed to block harmful research from getting into the wrong hands. The scientific community is looking toward the National Security Agency (NSA) to do just that. According to the NSA's values, the agency seeks to improve and modernize the security of sensitive information systems in an effort to protect against bioterrorism (NSA, 2013). Right now, our nation is limited to voluntary censorship of potentially harmful research. Critics say that it may not be enough (Selgelid, 2007).
Summary
In this chapter, we have described terrorism and emergency response in the past and present in the United States. We have identified the key agencies at various government levels that become involved during an emergency and discussed their roles in emergency response. In addition, we examined the eight principles of emergency management, as well as the National Incident Management System and specifically how it functions during times of disaster. The emergencies evaluated included those that are man-made and natural, as well as those labeled terrorist or bioterrorist attacks against the nation.
Disasters are bound to happen, but the most critical point from the public health standpoint is to prepare for the worst and hope for less. Regardless of what type of disaster occurs, the importance lies in solid plans for emergency response and preparedness.



