Health Information Systems and the Electronic Health Record

Completion of Neehr Perfect Scavenger Hunts Levels I and II.
Identify the differences between coded and non-coded data entry.
Identify the differences between structured and unstructured data entry.
Evaluate the clinical implications of structured versus unstructured data entry in the EHR.
Relate the use of coded data to meeting the objectives of the Meaningful Use effort for implementation of electronic health records.
Student instructions
If you have questions about this activity, please contact your instructor for assistance.
Document your answers directly on this document as you complete the activity. When you are finished, save this document and upload it to your Learning Management System (LMS). If you have any questions about submitting your work to your LMS, please contact your instructor.
Screen displays are provided as a guide and some data (e.g. dates and times) may vary.
Clinical Reminders: Clinical Reminders assist in clinical decision-making, improved documentation, and clinical follow-up by using performance measures and universal use of electronic health records. It’s a unique linkage with standardized, consistent performance measurements. The primary goal of clinical reminders is to provide relevant information to providers at the point of care, for improving patient care. Clinical reminders provide pertinent data for clinical decision-making, reducing duplicate documenting activities, assist in identifying patients, and contribute to compliance with performance measures and with Health Promotion and Disease Prevention guidelines.
Coded Data: Quantitative data entered into specific fields in the EHR via a computerized form which enables the search, retrieval and/or data mining of the gathered information. Examples of coded data include ICD diagnostic codes, CPT procedural codes, health factors, the order number for a medication and the numbered barcode associated with it.
Data mining: Compiling and reporting of data from coded fields within the EHR for accurate bio-surveillance, public health reporting, quality improvement and performance measurement.
Electronic Health Record (EHR): A longitudinal electronic record of patient health information that spans over time. This time could be a few months or many years. It is generated by one or more encounters in any care delivery setting. Included in this information are patient demographics, progress notes, problems, medications, vital signs, past medical history, immunizations, laboratory data, and radiology reports.
Encounter Form - A “form” in the EHR that is used to collect relevant information of a patient whenever visiting a healthcare facility. This form, or template, is used by the healthcare providers to minimize inconsistencies and validate entries for improved care, billing, and coding. Encounter forms are specific to each clinic and hospital ward and will look a little different depending on the patient’s location. The encounter form may contain some of the following for entering data: diagnoses, completed procedures or exams, documentation of immunizations, generating health factors, and so on. Some of the fields contain coded data and will populate other parts of the electronic health record when documented in.
Health factors: A health factor is a non-diagnostic, non-charge bearing type of coded data that captures patient health information for purposes of case-finding or tracking, such as Family History of Alcohol Abuse, Lifetime Non-smoker, No Risk Factors for Hepatitis C, etc.
Meaningful Use: Meaningful Use describes the use of health information technology (HIT) that leads to improvements in healthcare and furthers the goals of information exchange among health care professionals. To become Meaningful Users, health professionals need to demonstrate they're using certified EHR technology in ways that can be measured in quantity and in quality, such as the recording and tracking of key patient health factors to enable the planning and delivery of timely and effective care.
Query: A request for information from a database. Posing queries can be done by choosing parameters from a menu, specifying the fields and values that define the query, or by making the request written in a special query language.
Structured data: Information entered in a structured or pre-determined field within a record or file. This information, or data, is understood by other functions in the EHR because it is built with a universal set of protocols. These fields can be referenced or extracted by other parts of the EHR because they are in this structured format. Think of these fields as “talking” to one another, or as being “connected” by a set protocol. Examples of structured data: Patient date of birth and age, blood pressure, patient risk assessment questionnaire with multiple-choice answers, check boxes (“point and click”). The context of the data may determine whether or not the data is structured or unstructured—e.g., a progress note might be standardized and structured in some EHRs (e.g., Subjective/Objective/Assessment/Plan) fields, but unstructured in others.
Unstructured data: Information that is entered in an unstructured format, such as a nurse’s narrative note or the free text in a comments box. It is considered free form and does not follow any sort of organizational pattern, similar to typing a couple of sentences in a word document. The EHR is not able to easily read and interpret information that is free form.
The activityThe power of the EHR
The key to unlocking the powerful potential of the EHR is the careful and consistent entry of data into retrievable areas, or fields, also referred to as structured or coded data fields. Properly entered electronic health data enables search, retrieval, and comparison across patient populations over time in a process called data analysis. This carefully extracted data can be used for meaningful research to improve individual patient care, patient safety and best practices in healthcare delivery.
However, the EHR is only useful if the data entered by the user is correct and placed in structured and coded data fields. This is what makes the EHR “meaningful” in its function and capabilities. When data is entered correctly it has the potential to lower healthcare costs, improve patient safety and decrease healthcare errors. Keeping that in mind, not every piece of information must go into a structured or coded field. There is still a need for the unstructured comment boxes and notes. The unstructured areas “fill in the blanks” and enable the inter-professional use and coordination of patient care that is important in healthcare.
Structured and unstructured data entry fields
In the following screenshots are examples of structured and unstructured data fields that are found in the EHR. Any data entered in a structured field can easily be extracted, aggregated and summarized for easy interpretation in a standardized report.
Entering allergies in this format is structured data. The causative agent, or allergen, is coded data, meaning there is a code associated with each causative agent in the allergen file.

When selecting from the dropdown menus of Nature of Reaction and Signs/Symptoms, the selections cannot be altered. The EHR provides this fixed data in a structured format.

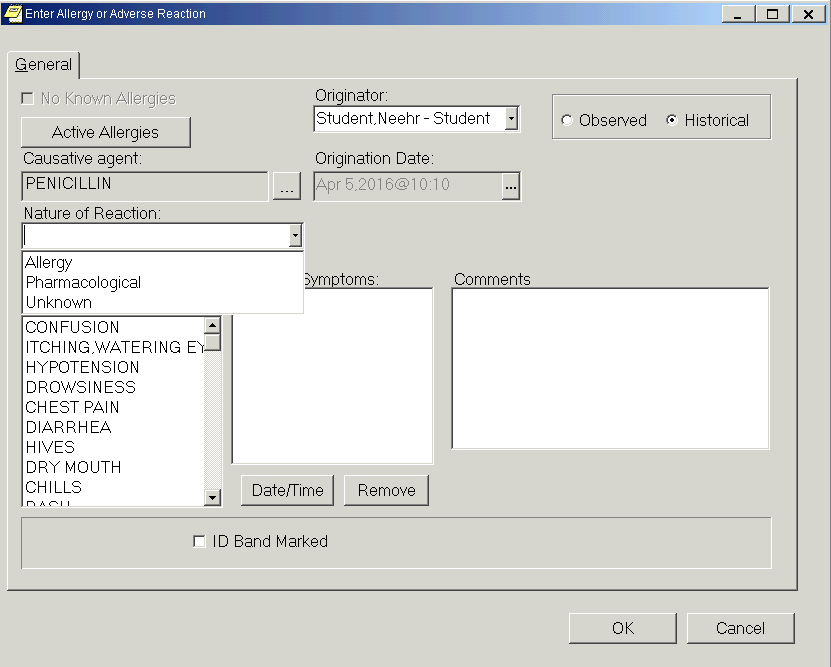
Structured data
Selecting signs and symptoms from the dropdown is structured data.


Structured data
Entering free text data in the Comments box is unstructured data.


Unstructured data
The note
Notes can be used to enter and report information about the patient or their care. Notes can be:
Untemplated – No structure in the body of the note, i.e. free text. The header and footer information will still be structured, even if the body of the note is free text.
Templated – Can be a combination of structured and unstructured components. Most of these structured fields are designed to make documenting in the note easier for the user. They generally cannot be coded for data mining or creating reports. Examples of structured fields are dropdown menus, check boxes, or selecting from a list. These types of fields do not allow the user to change the text or number of characters.
Templated with coded fields – Can contain a combination of structured, unstructured, and coded fields. These notes are designed so that the coded fields will generate data based on a universal protocol that the EHR recognizes. What it recognizes will be used to select the appropriate Clinical Reminder and/or Health Factor for the patient. Then there are coded data components that can pull in data from other parts of the chart (i.e., vital signs) to complete the note, or can populate other areas of the chart (i.e., home medication list).

Untemplated

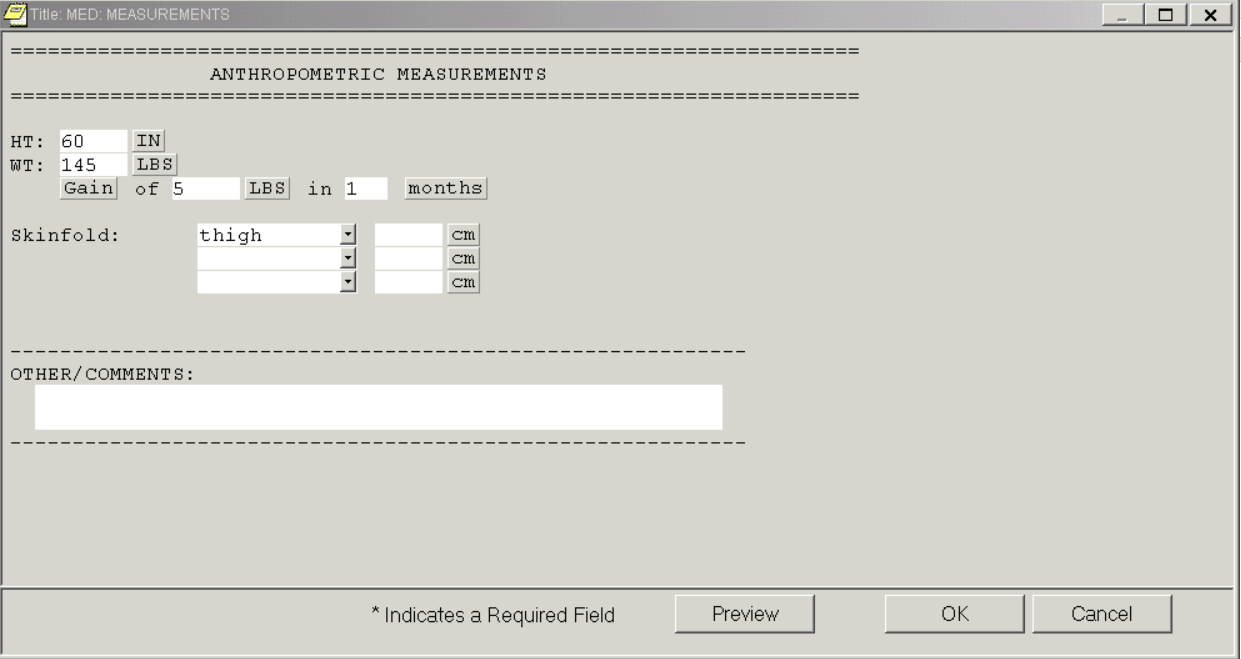
Templated
Unstructured data field
Structured data field



Clicking on the DVT Prophylaxis above triggered a Health Factor code. This will in turn show in the Encounter coding form.
This white area at the bottom indicates there are coded fields in the note.
Coded data field
Templated note with coded fields
Because of the design of most notes in an EHR, you cannot tell by looking at the final documented note if it has structured or coded fields in it. The way to determine this is to look at the template for a note, i.e. how the note is created.
Coded and non-coded data entry fields
Any data entered in a coded field can easily be searched, retrieved, aggregated and summarized for easy interpretation in a standardized report. The most obvious coded data found in the EHR are medical diagnosis codes (or a problem codes), procedure codes, exam codes, or demographic data codes. Other elements in the EHR that are also considered coded data include lab results, orders, allergies, and medications.
Problems
Diagnosis/Problems must be carefully entered for several reasons.
Correct diagnosis placed in chart
Appropriate treatment
Appropriate coding and billing
Accurate financial reimbursement
Data mining
The codes that “capture” the diagnosis or problem and transform the human readable words to alphanumeric codes that the EHR interprets are called ICD codes (International Statistical Classification of Diseases and Related Health Problems, 10th revision). ICD-10 codes are for coding of diseases, signs and symptoms, abnormal findings, complaints, social circumstances and external causes of injury or diseases, as classified by the World Health Organization (WHO).
Providers select the appropriate diagnosis and/or code based on the information they have gathered about the patient (assessment, interview, tests). With Neehr Perfect, there is an “unclassified” code, 799.9. This 799.9 code is automatically assigned if an ICD code is not available. The 799.9 code is reserved for an unidentifiable illness or diagnosis – its use is discouraged in practice. Even though it is the easiest thing to select and will save time with searching, it does not meet meaningful use standards nor will it be an ICD code that can be used in billing or reporting.

Correctly coded with ICD10 E118
Incorrect using 799.9

The Encounter Form
The Encounter Form is most often associated with outpatient use, such as at the doctor’s office. However, coding the Encounter Form for inpatient care is also valuable. As explained by the definition of the Encounter Form, certain parts of the form are coded and other elements are structured, therefore the data can be extracted and reported. The coded data can also be shared in other parts of the chart for immediate clinical use. In the following example of the Encounter Form, the diagnoses have been checked and identified as being Problem List Items. The EHR will recognize this data in the encounter form and will populate the designated areas of the chart where this information can be utilized by the healthcare team.

If you were to log in and view Mr. Frank Stratten’s chart in the EHR, you would find that once the encounter form was completed, the data began to populate other areas of the chart.
At the bottom of the note, Health History (Medical Office), is a structured and coded summarization of the Encounter Form:

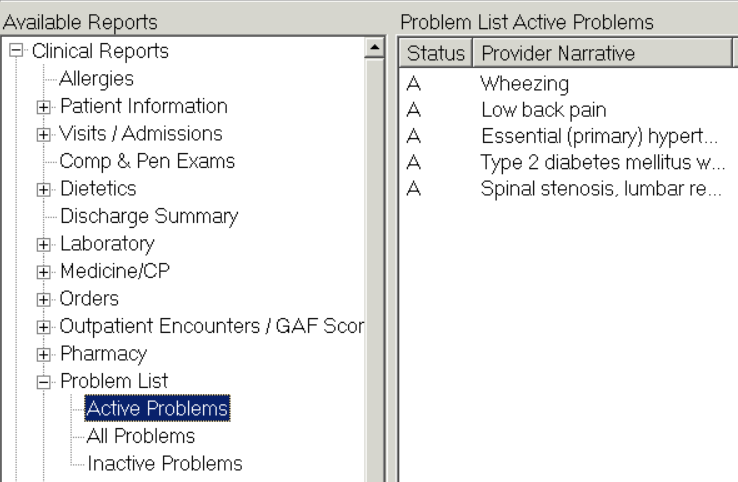
Data is shared on the Problems tab:

On the Cover Sheet:

And on the Reports tab of Mr. Stratten’s chart:
Simultaneously the EHR is also determining if these problems meet any of the criteria for Clinical Reminders or other Alerts that would be triggered for the provider.
Interaction with the Encounter Form allows the “backend” of the EHR, VistA, to become populated. Now Mr. Stratten’s information is being maintained by the EHR for the availability of data mining.
Real-life application
A medical office is beginning a new project to identify patients at risk for a heart attack or stroke. The HIT manager is asked to generate a report of all of the adults over 30 years old that come to the medical office with hypertension, type 2 diabetes, who smoke, and/or have a BMI over 25. The data needed to generate this information is in the EHR. It has been documented in each person’s chart. But it isn’t practical to look through each individual chart. Generating a report from the EHR master patient index (MPI) is much more efficient. To gather what is needed, the correct information must have been entered in structured and coded fields and the correct “questions” must be asked of the EHR when building the query. In other words, how the query is entered in the EHR will determine if the correct data is extracted. The following screen shots demonstrate how data is queried in the VistA EHR, then extracted and placed in an excel spreadsheet.
Following is a screen shot of the MPI query tool of the EHR, VistA. This is where data mining occurs.

Once the information is gathered in VistA it can be extracted and placed in a spreadsheet or database tool for easier sorting and viewing.
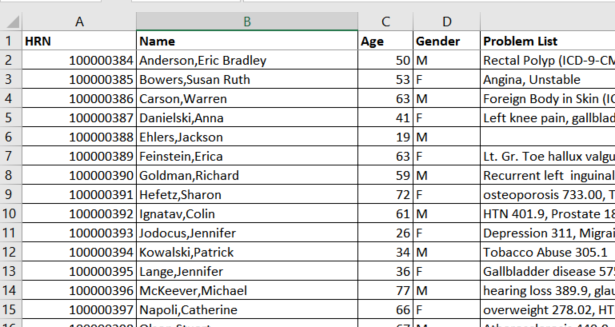
The information can then be used to set the objectives of the project, determine interventions, look at trends, compare to state and national numbers, develop policy and much more.

Structured and coded data improves patient safety
A patient’s allergies to medications are important to consider when ordering and administering medications. EHRs have multiple safety checks to remind the healthcare provider of an allergy. Meaningful use has stressed this even more by requiring that a current allergy list always be maintained as one of the core objectives. In order for the EHR to send alerts and perform safety checks, the allergy must be entered in the correct place – a field that is structured or coded.

Structured data


An untemplated note (a free text note)
Results in Unstructured data
Postings
On the Cover Sheet in the upper right corner is a box titled Postings. Postings contain important patient-related information of which hospital staff and medical office personnel need to be aware. The postings box can contain notes from the notes tab, allergies, warnings, and advance directives. Postings are coded data that can be extracted through VistA to generate reports.
Some notes have been developed so that when they are completed by the user they will not only show on the Notes tab but also in the Postings box. The note has been identified as containing critical information to the patient’s care and/or safety; for example, lab results, code information, advance directives, suicide attempts. On a larger scale, if you wanted to know how many, or which, charts have an Informed Consent form documented you could run a report in VistA.
Some postings are created automatically when data is entered in a particular coded or structured field. When allergies are entered, the EHR will display “Allergies” information about medications, foods, and other items to which patients are allergic or to which they may have an adverse reaction.
Medication orders and medication administration are another area of patient safety that impact patient care and the EHR. Once an order is entered in a patient’s EHR, it is coded. It is assigned an order number allowing it to be tracked and associated with that order and the patient. No two order numbers in an EHR system will be alike. This medication order number is also linked with the barcode assigned to it. Each medication dose has its own unique barcode. This barcode is what is scanned by the healthcare professional to document that the specific medication and dose is being administered to the patient.


Medication barcode
Labs are also assigned coded data. This lab number allows this particular lab to be tracked in the patient’s chart and through the EHR.

Clinical Reminders are health promotion and disease prevention needs identified for the patient, based on relevant structured or coded data pre-programmed to be included in a reminder query, and possibly trigger a specific reminder to be scheduled.
Clinical Reminders are displayed based on information entered in the correct structured field. The EHR looks at the patient age, sex, problems, vital signs, and data entered into specially developed notes. For example, in Mr. Stratten’s chart, when the user enters his weight and height at the clinic, the EHR takes that information, formulates the BMI and generates the BMI Clinical Reminder if the BMI is out of a pre-specified range.

Structured, coded, and free text data fields can be found on almost every tab of the EHR. One of the key benefits to the electronic health record over paper health records is the ability to retrieve data. However, just because information is entered electronically doesn’t automatically make it retrievable or meaningful.
To complete the activity, log in to the EHR and access the Frank Stratten and Eva Tatters charts to answer the following questions. Use of the skills learned in Scavenger Hunts I and II will help navigate the charts.
First, access the EHR chart of Eva Tatters.
Which of the following active problems in Mrs. Tatters’ chart is entered correctly as coded data and would meet meaningful use standards?
Pain
Essential (primary) hypertension
Osteoarthritis knee
None of them
When the problem is entered correctly in the patient chart, what can be accomplished with that information?
Financial reimbursement will be expedited.
The coded and non-coded data can be sorted and extracted for training purposes.
The patient will receive appropriate treatment.
The Health Factors will be updated.
Mrs. Tatters has a History and Physical written the day she arrives to the hospital. This note is an unstructured, non-coded note. There are several discrepancies with what is written in this note and what has been documented in other places of the chart. Which of the following statements is true?
Labs are entered on the Cover Sheet and in the Labs tab.
The allergy listed in the note is different from the allergy on the Cover Sheet.
She has active medications ordered.
She has been diagnosed with secondary hypertension.
Mrs. Tatters is allergic to Latex. Is Latex entered into a structured or unstructured field?
Structured
Unstructured
You are asked to complete a note in Mrs. Tatters chart. When you open it the note has all check boxes for entering the data. These check boxes are:
Structured
Unstructured
Mrs. Tatters has two medical problems entered in the EHR with 799.9 codes, pain and osteoarthritis of the knee. Which of the following statements is correct?
These are also mentioned in the history and physical so they are already coded correctly.
It’s okay to use the 799.9 code for the problem of pain to save time.
The 799.9 code should not be used because it is not specific enough for coding and billing purposes.
All of the above.
Mrs. Tatters has four sets of vital signs entered in her chart. However, they are not all located in the same place in her chart. This could result in an inaccurate interpretation of her health status, as well as be difficult to data mine and extract, or demonstrate meaningful use of the EHR. Select the correct statement:
The data entered in the notes is the most current and accurate information.
The data entered in the Vitals section of the Cover Sheet is always entered correctly. This means that it can be data mined and meets meaningful use standards.
The Vital Signs should all be entered in the Vitals section of the Cover Sheet, where they are placed in structured and coded data fields. These fields can be graphed and data mined.
The Vital Signs should all be entered in the NURS: PROGRESS NOTE for consistency.
Postings are created automatically when data is entered in a particular coded or structured field in another area of the chart. Postings can contain crucial information about the patient that the user needs to be aware of. Which of the following statements is the most accurate?
A posting can list what medications the patient is allergic to.
The Lab Results Note in the Postings will only list labs that are abnormal.
A patient’s favorite foods will be listed in Postings.
Postings will only list non-coded and unstructured information not found in other areas of the chart.
Using File > Select New Patient, open Mr. Stratten’s chart.
Look at Mr. Stratten’s chart. Which of the following statements is true?
The glucose POC lab has a lab code assigned to it.
The problem ‘low back pain’ has an ICD10 code of M545 assigned to it.
The medication order for the cefazolin has a coded order number assigned to it.
All of the above.
The active problem ‘Spinal Stenosis, Lumbar Region’ is an example of coded data.
True
False
Mr. Stratten has several Clinical Reminders in his chart that meet meaningful use standards. Which of the following statements is true?
The Body Mass Index reminder is set to prompt for a person with a BMI greater than 23.
The Body Mass Index reminder is set to prompt for women before men.
The Lipid Measurement reminder is set to prompt for a lipid panel every 5 years between the ages of 35 and 50 for men.
The Lipid Measurement reminder is set to prompt for a lipid panel every 5 years when the patient has diabetes.
The note, Release of Information Form, is also ________________ .
A posting
Coded data
A Clinical Reminder
A safety warning to the staff
In the Release of Information note there is structured and unstructured data. Which of the following is defined as the structured data in the note?
a. The purpose of the release
b. The address for Dr. Twelve
c. The fax number for Ridgeview Orthopedics
d. Checked box indicating which health records were released
Identifying and listing a current allergy in a coded data entry field in Mr. Stratten’s chart will produce multiple safety checks in the EHR to remind the healthcare provider of his allergies.
True
False
A report from VistA can be generated that includes all patients diagnosed with lung cancer by identifying any mention of lung cancer in the health history note.
True
False
A report from VistA can be generated that includes all patients diagnosed with lung cancer by identifying any ICD-10 codes of lung cancer entered as a Problem in the patient chart.
True
False
Which of the following statements is the most accurate?
Once an order is entered in a patient’s EHR, it is coded.
Clinical Reminders are displayed based on information entered in the correct structured field.
The EHR is not able to easily read and interpret information that is free form.
All of the above.
Which of the following statements is the most accurate?
An Encounter Form is used to minimize inconsistencies and validate entries to maximize patient insurance benefits.
Coded data is entered into specific data entry fields which enables the search, retrieval and/or data mining of the gathered information.
Unstructured data can be entered in structured data entry fields and then edited.
Data entered in structured data entry fields cannot be extracted by other parts of the patient chart.
| 16 | Neehr Perfect Level III Scavenger Hunt: The Power of the EHR v6 Archetype Innovations, LLC ©2017 |



